Hormone replacement therapy (HRT) is a treatment that replaces the estrogen, and usually the progesterone, that the body makes less of around menopause, and it remains the most effective option for hot flashes, night sweats, and other menopause symptoms [1][3]. That, in plain terms, is what HRT means. This guide explains the medical abbreviation, how the therapy works, who it is for, the types and forms, the real benefits and absolute risk numbers, what the 2024 Women's Health Initiative follow-up changed, and how to start. It is written to be a neutral, guideline-anchored reference, not medical advice, and it links out to deeper guides on every sub-topic. If you want the fuller companion piece on the female experience specifically, see our guide to HRT for women.
🔑 Key Takeaways
- Hormone replacement therapy replaces declining hormones, mainly estrogen (with progesterone added when you still have a uterus), and it is the most effective treatment for menopausal hot flashes and night sweats [1][3].
- The people who benefit most are generally under 60 or within 10 years of their final period, which clinicians call the timing window or window of opportunity [6][8].
- The main risk headline, in absolute terms, is small: the large WHI combined-therapy arm found roughly 8 extra breast cancer cases per 10,000 women per year, and Cleveland Clinic frames the added risk as less than 1 in 1,000 women per year [2][5][11].
- The 2024 long-term WHI follow-up reshaped the risk picture, reporting no increase in breast cancer or cardiovascular deaths and lower all-cause mortality when therapy started under 60 or within 10 years of menopause [6][8].
- HRT is an individual decision made with a clinician, who weighs your age, symptoms, health history, and preferences rather than applying a one-size rule [1][7].
Quick Stats
| Figure | What it means |
|---|---|
| About age 51 | Average age of natural menopause in the United States [3] |
| 3 to 4 weeks | Typical time for hot flashes and night sweats to ease after starting HRT [8] |
| About 5 years or less | Common length of use, though there is now no fixed time limit [2][7] |
| About 3 percent | Share of candidate women currently using hormone therapy, largely out of fear [8] |
What Is HRT? HRT Meaning and Medical Abbreviation
HRT is a medical abbreviation, and what HRT stands for is hormone replacement therapy. If you searched "whats HRT" or "what is HRT?", the short answer is a prescription treatment that tops up the estrogen and progesterone your ovaries make less of as they wind down toward menopause [1][3]. The goal is to relieve symptoms driven by that hormone drop, from hot flashes to vaginal dryness, using the lowest dose that works for you [4].
You will increasingly see clinicians use newer names. Both Mayo Clinic and Cleveland Clinic now favor "menopause hormone therapy" (MHT) or simply "hormone therapy" (HT), and they stress that these terms mean the same thing as HRT [1][2]. The name shifted because "replacement" implied the goal was to restore youthful hormone levels, when the actual aim is symptom relief at a modest dose [1]. There is also an age nuance worth knowing: Cleveland Clinic notes the label HRT is often used more specifically for people in premature or early menopause (before age 40), while HT and MHT cover the broader menopause group [2].
One quick disambiguation, because search engines mix these up. In psychology, HRT can also stand for habit reversal training, a behavioral therapy for tics and body-focused repetitive behaviors. That is an entirely unrelated field. Everything on this page refers to hormone replacement therapy for menopause and related hormone needs.
How HRT Therapy Works
To understand how HRT therapy works, start with what changes at menopause. During perimenopause and then menopause, the ovaries produce far less estrogen and progesterone, and it is that decline, especially the fall in estrogen, that drives hot flashes, night sweats, disrupted sleep, mood changes, and vaginal and urinary symptoms [1][3]. HRT hormone therapy works by supplying a steady, low dose of estrogen (and progesterone when needed) so that the brain thermostat, vaginal tissue, and other estrogen-sensitive systems settle back down [3].
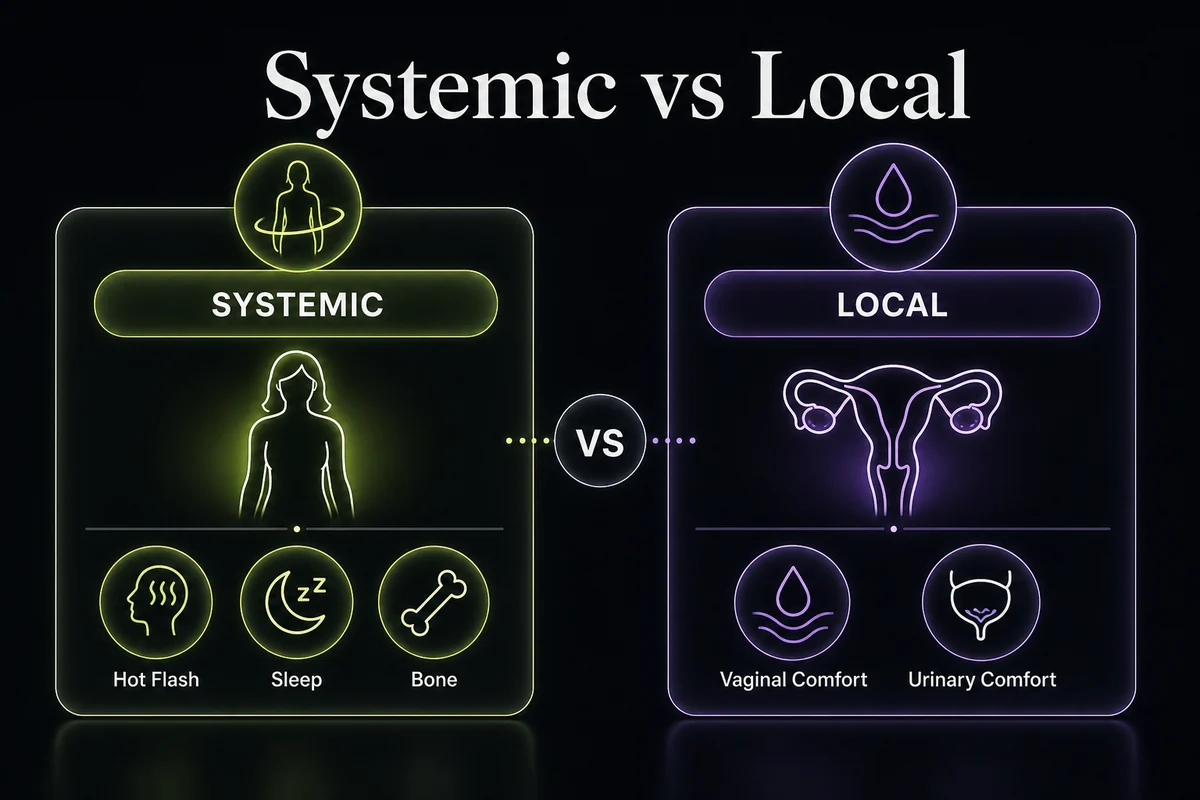
Delivery matters as much as the hormone itself. ACOG frames this as systemic versus local. Systemic therapy (pills, patches, gels, sprays, and the higher-dose vaginal ring) sends estrogen through the whole body and treats the full range of symptoms, including hot flashes and bone loss [3]. Local therapy (low-dose vaginal creams, tablets, or a low-dose ring) acts mainly on vaginal and urinary tissue with very little reaching the bloodstream, which makes it a targeted option for dryness and painful sex [3][1]. If you still have a uterus, systemic estrogen is paired with a progestogen to protect the uterine lining, a point covered in detail below [3].
Who Is Hormone Replacement Therapy For?
Hormone replacement therapy is used by several different groups, and the intent behind your search shapes the answer. The largest group is women in perimenopause and menopause with bothersome symptoms. If that is you, our dedicated guides to HRT in perimenopause and HRT for menopause go deeper than this overview, and our companion article on HRT for women covers the female experience end to end.
A second group is people with early or surgical menopause. When menopause happens before about age 45, whether naturally, after surgery to remove the ovaries, or from certain treatments, Mayo Clinic notes that hormone therapy is generally recommended at least until the typical age of menopause, because it protects bone and cardiovascular health during years the body would normally still be making estrogen [1]. This is a case where the benefits are especially favorable.
A third group is men with diagnosed low testosterone. Male hormone therapy is a separate pathway usually called testosterone replacement therapy (TRT), prescribed for men with clinically low testosterone confirmed on blood tests and symptoms, and it works differently from estrogen-based HRT. We keep it brief here and cover it fully in our guide to HRT for men.
Finally, hormone therapy is also part of gender-affirming care for transgender and nonbinary people, prescribed and monitored by specialized clinicians. We do not cover those protocols here; for reputable, specialist guidance, the UCSF Gender Affirming Health Program (transcare.ucsf.edu) is a widely cited resource.
Types of HRT: Estrogen, Progesterone and Testosterone
At the highest level, HRT treatment comes in two core setups: estrogen alone, used by women who no longer have a uterus, and estrogen combined with a progestogen, used by women who still have a uterus [3][1]. Within those, the hormone can be delivered several ways. This section is an overview; for the deep dive, see all the types of HRT compared.
Estrogen therapy
Estrogen is the workhorse of HRT and the hormone that relieves most menopause symptoms. Estrogen-only therapy is prescribed for women who have had a hysterectomy, because without a uterus there is no lining to protect [3]. HRT estrogen comes as pills, skin patches, gels, sprays, and vaginal preparations (ring, cream, or tablet), and the same estradiol can be given locally in low doses purely for vaginal and urinary symptoms [1][3]. Patches, gels, and sprays are absorbed through the skin and, unlike HRT pills taken by mouth, do not pass through the liver first, which is why they carry a lower blood clot risk [1][3]. Our guide to how HRT patches work covers the transdermal route in detail.
Progesterone HRT: why it is added
If you still have a uterus, estrogen is combined with a progestogen, and this is where progesterone HRT comes in. The reason is protective: unopposed estrogen thickens the uterine lining and raises the risk of endometrial (uterine) cancer, and adding a progestogen keeps the lining thin and offsets that risk [3][1]. Progesterone for HRT can be given continuously (a little every day, aiming for no monthly bleed, often preferred after menopause) or cyclically (in a monthly pattern that produces a scheduled bleed, often used in perimenopause) [2]. Many clinicians use oral micronized progesterone taken at night, partly because it can have a mild calming effect that helps sleep [8]. Our HRT dosage chart shows how these are typically combined.
Testosterone: HRT vs TRT
The difference between HRT and TRT trips people up. In everyday use, HRT usually means estrogen and progesterone therapy for menopause, while TRT means testosterone replacement for men with diagnosed low testosterone. For women, testosterone is sometimes used off-label for low sexual desire, but Stanford notes it is not FDA-approved for women and the evidence is mainly for libido rather than energy or mood [8]. For men, TRT is a different clinical pathway with its own workup and monitoring, which we cover in HRT for men.
The table below compares the common forms of HRT. No competitor page on this topic includes one.
| Form | Hormone(s) | Systemic or local | Typically used for | Notes |
|---|---|---|---|---|
| Oral pill | Estrogen, or estrogen plus progestogen | Systemic | Hot flashes, night sweats, mood, bone protection | Convenient; passes through the liver, so slightly higher clot risk (for example Premarin, Estrace) [1][3] |
| Skin patch | Estradiol (progestogen added or combined) | Systemic | Same as oral, with steadier day-to-day levels | Lower clot risk than tablets (patch-class products such as Climara, Vivelle-Dot) [1][3] |
| Gel or spray | Estradiol | Systemic | Same as patch | Daily application; dose is easy to fine-tune (for example EstroGel, Evamist) [1][3] |
| Vaginal ring | Estradiol (low-dose local, or higher-dose systemic) | Local or systemic | Vaginal dryness and urinary symptoms; systemic ring also treats hot flashes | Low-dose local ring (Estring) treats local symptoms only; a systemic ring (Femring) treats the whole body [1][3] |
| Vaginal cream or tablet | Estrogen | Local | Vaginal dryness, painful sex, urinary symptoms | Minimal amount reaches the bloodstream (for example a vaginal tablet such as Vagifem) [1][3] |
| Progestogen (oral micronized progesterone, or levonorgestrel IUD off-label) | Progesterone or progestin | Systemic (IUD acts locally) | Protects the uterine lining when estrogen is used | Micronized progesterone often taken at night; a levonorgestrel IUD is used off-label for lining protection per WebMD [8][3] |
Brand names are examples only and are shown sparingly; your clinician chooses the product and dose. See all the types of HRT compared for the full menu.
Benefits of HRT
The benefits of HRT are best understood as symptom relief plus a few longer-term protections, all weighed against the risks in the next section. For the fuller balance sheet, see our guide to the pros and cons of HRT.

The headline benefit is vasomotor symptoms. ACOG describes systemic hormone therapy as the most effective treatment for hot flashes and night sweats [3]. Beyond that, estrogen relieves genitourinary symptoms of menopause (vaginal dryness, irritation, painful sex, and some urinary symptoms), and by easing night sweats it often improves sleep, which in turn steadies daytime mood and energy [1][3]. Many women also report relief of menopausal joint aches, a benefit Stanford lists among the effects of restoring estrogen [8].
There is also a recognized bone benefit. Systemic estrogen slows the bone loss that speeds up after menopause, and it is an FDA-approved option for preventing postmenopausal osteoporosis in appropriate candidates [3][7]. Our guide to HRT and osteoporosis covers this in depth. ACOG also notes a possible reduction in colon cancer risk with combined therapy, though this is not a reason on its own to start [3]. The tone that guidelines take is measured: HRT treats symptoms and protects bone, but it is not marketed as a cure-all or an anti-aging drug [1][7].
Risks and Side Effects of HRT
The risks of HRT are real but often misunderstood, and they depend heavily on your age, the type of therapy, the route, and how long you use it [1][6]. This is an overview; for depth, see our full guide to HRT side effects and our explainer on HRT and breast cancer risk, explained with absolute numbers.
The most discussed risks are breast cancer, blood clots, stroke, endometrial cancer, and gallbladder disease [1][3]. Two rules put them in perspective. First, timing: risks are lowest when therapy starts before age 60 or within 10 years of menopause, and they rise when it starts later [6][8]. Second, route: oral estrogen carries a small extra clot and stroke risk because it passes through the liver, while transdermal estrogen (patch, gel, or spray) keeps clot risk close to baseline, which is why ACOG and Stanford highlight the transdermal route for people with clot risk factors [3][8]. Estrogen given alone raises endometrial cancer risk, but adding a progestogen offsets that, which is exactly why combined therapy exists [3].
Some people should generally not use systemic HRT, including those with a history of breast cancer, certain other hormone-sensitive cancers, unexplained vaginal bleeding, active liver disease, or a history of blood clots or stroke, unless a specialist decides otherwise [4][1]. Common early side effects, such as breast tenderness, bloating, nausea, headaches, and irregular spotting, usually settle within the first few months as the body adjusts [2]. Clinicians can also use formal decision-support tools to weigh your individual risk; the Menopause Society's MenoPro app is one example that some providers use during the conversation, and it functions like an HRT risk calculator rather than a substitute for clinical judgment [7].
The table below puts the main risks in absolute terms. Absolute numbers, not relative percentages, are the honest way to read risk.
| Outcome | Roughly how common without HRT | With combined HRT | Key modifier |
|---|---|---|---|
| Breast cancer | Background risk rises with age and family history | About 8 extra cases per 10,000 women per year in the WHI combined arm; the estrogen-only arm showed a decrease | Risk grows with longer combined use; Cleveland Clinic frames added risk as less than 1 in 1,000 women per year [2][5][11] |
| Blood clots (venous thromboembolism) | Uncommon at baseline | Higher with oral estrogen; close to baseline with transdermal | Route matters most; patches and gels avoid most of the added risk [3][6] |
| Stroke | Low, rises with age | Small absolute increase, mainly with oral estrogen and older starters | Lower when started in the timing window and by non-oral routes [6] |
| Endometrial (uterine) cancer | Low | Not increased when a progestogen is added; increased with estrogen alone | Adding progestogen is what offsets the risk [3][1] |
| Gallbladder disease | Uncommon | Modest increase, more with oral therapy | Transdermal routes appear lower risk [1][3] |
Every figure above is drawn from the cited sources; nothing is invented, and individual risk varies. Your clinician will personalize these numbers to your history.
What the Research Says: WHI Then and Now
The biggest HRT news of the past two decades is the reinterpretation of one study. In 2002, the Women's Health Initiative (WHI) combined-therapy trial was stopped early after reporting increased risks, and headlines drove a wave of fear that cut HRT use sharply [11][8]. What often got lost is what the trial actually studied. The average participant was about 63 years old, well past menopause, and the therapy was a specific oral formulation (conjugated equine estrogen plus medroxyprogesterone) [11][6]. In other words, it tested one regimen mostly in older women, not HRT started in the timing window by symptomatic women in their 50s.
The picture has since been refined by long-term follow-up. In May 2024, JAMA published a 20-year review of the WHI trials led by Manson and colleagues, and Stanford's menopause program summarizes the takeaways clearly: no increase in breast cancer or cardiovascular deaths over the long term, and lower all-cause mortality when hormone therapy was started under age 60 or within 10 years of the final period [6][8]. That is why modern guidance from the Menopause Society individualizes the decision by age, symptoms, and health history rather than applying a blanket warning [7]. As Stanford notes, only about 3 percent of women who are candidates currently use hormone therapy, a gap that clinicians attribute largely to lingering fear from the 2002 era [8].
HRT Before and After: What to Expect and When
People search "HRT before and after" hoping for a realistic timeline, so here is an honest one. HRT is gradual, not instant, and different symptoms improve on different schedules [8][2]. Hot flashes and night sweats are usually the fastest to respond; Stanford puts meaningful relief at about 3 to 4 weeks [8]. Sleep, mood, and vaginal symptoms tend to keep improving over the following couple of months, while skin and libido are slower still [2][8]. For a fuller week-by-week breakdown, see our guide to how long HRT takes to work.
It is just as important to say what HRT does not do. It is not a direct weight-loss drug, and expecting the scale to drop simply from starting it sets up disappointment; any change in body composition is modest and tied to better sleep and activity rather than the hormone burning fat, a point our guide on does HRT cause weight gain explains. Some women do notice a shift in where fat sits and a bit less bloating over time, but this should be framed cautiously, not sold as a body transformation.
| Timeframe | What typically changes |
|---|---|
| Weeks 1 to 2 | Hormone levels stabilize; mild settling-in effects possible (breast tenderness, spotting, nausea) [2][9] |
| Weeks 3 to 4 | Hot flashes and night sweats often begin to ease [8] |
| Months 2 to 3 | Sleep, mood, and vaginal and urinary symptoms continue to improve [2][8] |
| Months 3 to 6 | First formal dose review; slower symptoms such as skin and libido catch up [7] |
| 1 year and beyond | Bone-protective benefit accrues while therapy continues [7] |
Treat these as typical ranges, not guarantees; see how long HRT takes to work for the detail.
How to Start HRT
If you are wondering how to start HRT, the process is more straightforward than it looks, and it follows a few clear steps.
1. Take a symptom inventory. Write down what is bothering you most (hot flashes, sleep, mood, vaginal dryness, joint aches) and how much it affects daily life. This focuses the whole conversation [1]. 2. Review your medical history. A clinician will ask about your age, time since your last period, and any history of breast or hormone-sensitive cancer, blood clots, stroke, liver disease, or unexplained bleeding, which are the main reasons HRT might not be suitable [4][1]. 3. Know when labs are and are not needed. In women over 45, menopause is a clinical diagnosis based on symptoms and cycle changes, so routine blood tests are often unnecessary; tests such as FSH are used selectively, for example in younger women or unclear cases [3][4]. 4. Choose a route and start low. Guidelines favor the lowest effective dose, adjusted over time, with transdermal options often preferred when clot risk is a concern [4][3]. 5. Plan follow-up. Expect a review at roughly 3 to 6 months to check how you are responding and to adjust the dose, then periodic (often annual) reviews after that [4][7].
You can start through an in-person route (a primary care clinician, OB/GYN, or a menopause specialist; the Menopause Society keeps a practitioner directory) or through telehealth, which many people find faster and more convenient. To see how the online route works, read how to get HRT online, and to find in-person options near you, see HRT doctors near me. Cost is a common question at this stage; our guide to what HRT costs breaks down prices with and without insurance.
Alternatives to HRT
HRT is not the only path, and alternatives matter for people who cannot or prefer not to use hormones. On the prescription side, newer nonhormonal medicines target hot flashes directly, including fezolinetant and the newer elinzanetant (a class of drugs that act on the brain's temperature-control pathway), alongside older options such as low-dose paroxetine and gabapentin, all prescribed and monitored by a clinician [10][3]. For vaginal symptoms specifically, nonhormonal vaginal moisturizers and lubricants can help, and low-dose local estrogen remains an option with minimal systemic absorption [3][1].
Lifestyle measures (regular exercise, limiting alcohol and triggers, layered clothing, and good sleep habits) can ease symptoms and support overall health, though they rarely match HRT for moderate to severe hot flashes [1]. On supplements and phytoestrogens, ACOG is candid that few have strong evidence, so they should be approached with realistic expectations [3]. A specific caution applies to compounded and pellet hormones: FDA-approved bioidentical hormones do exist and are well studied, but custom-compounded preparations and hormone pellets are not recommended by ACOG or the Menopause Society because of inconsistent dosing and safety concerns [3][7]. Our guides to bioidentical HRT and HRT pellet therapy cover this in detail.
For readers exploring the wider menopause toolkit, we also cover peptides for menopause and tirzepatide's off-label uses, which sit outside standard hormone therapy and should be discussed with a clinician rather than self-started.
Frequently Asked Questions
Related Reading
- How to get HRT online: how telehealth HRT prescriptions work. - What HRT costs: prices with and without insurance. - All the types of HRT compared: the full menu of options and forms. - HRT for women: the complete companion guide. - Stopping HRT safely: what to expect if you taper off.
References
- Mayo Clinic. Hormone therapy: Is it right for you? Accessed 2026. https://www.mayoclinic.org/diseases-conditions/menopause/in-depth/hormone-therapy/art-20046372
- Cleveland Clinic. Hormone Therapy for Menopause Symptoms. Accessed 2026. https://my.clevelandclinic.org/health/treatments/15245-hormone-therapy-for-menopause-symptoms
- American College of Obstetricians and Gynecologists (ACOG). Hormone Therapy for Menopause. Accessed 2026. https://www.acog.org/womens-health/faqs/hormone-therapy-for-menopause
- MedlinePlus. Hormone Replacement Therapy. U.S. National Library of Medicine. Accessed 2026. https://medlineplus.gov/hormonereplacementtherapy.html
- American Cancer Society. What to Know About Hormone Replacement Therapy and Cancer Risk. Accessed 2026. https://www.cancer.org/cancer/latest-news/what-to-know-about-hormone-replacement-therapy-and-cancer-risk.html
- Manson JE, Crandall CJ, Rossouw JE, et al. The Women's Health Initiative Randomized Trials and Clinical Practice: A Review. JAMA. 2024;331(20):1748-1760. https://jamanetwork.com/journals/jama/fullarticle/2818206
- The 2022 Hormone Therapy Position Statement of The North American Menopause Society (The Menopause Society). Menopause. 2022;29(7):767-794. https://pubmed.ncbi.nlm.nih.gov/35797481/
- Stanford Lifestyle Medicine. Menopause Hormone Therapy is Making a Comeback: Is It Safe and Right for You? Accessed 2026. https://lifestylemedicine.stanford.edu/menopause-hormone-therapy-is-making-a-comeback-is-it-safe-and-right-for-you/
- NHS. Hormone replacement therapy (HRT). Accessed 2026. https://www.nhs.uk/medicines/hormone-replacement-therapy-hrt/
- U.S. Food and Drug Administration. Menopause: Medicines to Help You. Accessed 2026. https://www.fda.gov/consumers/free-publications-women/menopause-medicines-help-you
- Writing Group for the Women's Health Initiative Investigators. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women. JAMA. 2002;288(3):321-333. https://pubmed.ncbi.nlm.nih.gov/12117397/
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.