The pros and cons of HRT come down to a single trade-off: hormone replacement therapy is the most effective treatment there is for menopause symptoms, and it carries real but small, quantifiable risks that depend mostly on your age, your health history, and the type you take. For most women who start before age 60 or within 10 years of menopause, the benefits usually outweigh the risks [1][5]. For women with certain cancer, clot, or liver histories, the balance tips the other way. This guide puts the benefits and the risks side by side with real numbers, then shows how age, hormone type, and delivery route move the needle, so you and your clinician can weigh them for your own situation rather than for an average patient.
HRT by the numbers:
| Quick fact | What it means |
|---|---|
| Under 60 or within 10 years of menopause | The window where benefits usually outweigh risks for most women [1][5] |
| About 5 extra breast cancer cases per 1,000 | Added over 5 years of combined HRT, compared with women not taking it [1] |
| No measurable clot increase | With transdermal estrogen (patch, gel, or spray) versus oral tablets [1] |
| Around 5 years, individualized | A common length of use, reviewed at least yearly, with no fixed cutoff [3] |
🔑 Key Takeaways
- HRT is the most effective symptom treatment available. Nothing else matches systemic estrogen for hot flashes, night sweats, and the sleep disruption they cause [1][5].
- The main risks are small and quantifiable. About 5 extra breast cancer cases per 1,000 women over 5 years of combined HRT, plus a small clot and stroke increase that is mostly tied to oral tablets [1].
- Type and route change the risk picture. Transdermal estrogen avoids the clot signal, and low-dose vaginal estrogen carries essentially no systemic risk [1][2].
- Age and timing matter most. Starting before 60 or within 10 years of menopause is the favorable window; early menopause before 45 is a reason to use HRT, not to avoid it [1][5].
- Some people should not take it. Prior hormone-sensitive cancer, blood clots or stroke, active liver disease, or unexplained vaginal bleeding usually shift the balance against HRT [1][3].
What Is HRT and Who Is It For?
Hormone replacement therapy replaces the estrogen (and often progesterone) that the ovaries stop making at menopause. There are two main forms. Estrogen-only HRT is used by women who have had a hysterectomy. Combined HRT, which adds a progestogen to the estrogen, is used by women who still have a uterus, because estrogen on its own thickens the uterine lining and raises the risk of endometrial cancer; the progestogen protects that lining [4][3]. HRT is primarily for women with bothersome menopause symptoms, and it is also standard care for early or premature menopause, where it protects long-term health until the usual age of menopause. For a broader primer on formulations and how treatment is started, see our complete guide to hormone replacement therapy and our HRT for women overview.
HRT Benefits vs Risks at a Glance
The fastest way to weigh HRT is to see the upside and the downside in one place. The table below pairs each benefit against the cost that sits closest to it, with an evidence grade in parentheses so you can tell what is firmly established from what is still uncertain. One principle runs through the whole table: the same therapy is safer the earlier in menopause you start it and the more you lean toward non-oral routes [1][2].
| Pros of HRT | Cons of HRT |
|---|---|
| Relieves hot flashes and night sweats (strong) | Small breast cancer increase with combined HRT (established, about 5 per 1,000 over 5 years) |
| Treats vaginal dryness and painful sex (strong) | Clot risk with oral tablets (established, avoidable by using a patch, gel, or spray) |
| Prevents bone loss and fractures (strong) | Small stroke increase with oral forms (established) |
| May support mood and sleep through symptom relief (moderate) | Side effects in the first months: breast tenderness, bloating, spotting (common, usually transient) |
| Possible heart benefit when started early (mixed, timing-dependent) | Endometrial cancer if estrogen is unopposed (established, prevented by adding a progestogen) |
| Recommended after early or premature menopause (strong) | Not suitable with certain cancer, clot, or liver histories (contraindication) |
The rest of this guide unpacks each row with the numbers behind it.
Benefits of HRT: What the Evidence Shows
The benefits of HRT range from very well established (symptom relief and bone protection) to genuinely uncertain (dementia and long-term heart protection). Grading them honestly is the point of this section.
Relief From Hot Flashes, Night Sweats, and Sleep Problems
Systemic estrogen is the single most effective treatment for vasomotor symptoms, the hot flashes and night sweats that define menopause for many women, and most people notice improvement within days to weeks of starting [1][5]. Because night sweats are a major cause of broken sleep in midlife, the sleep benefit tends to follow the symptom benefit rather than being a separate drug effect. Evidence grade: strong.
Vaginal Dryness, Painful Sex, and Urinary Symptoms
The tissue changes grouped under genitourinary syndrome of menopause, including vaginal dryness, painful sex, and some urinary symptoms, respond well to estrogen [1][4]. These can be treated with low-dose vaginal estrogen, which acts locally with minimal absorption into the bloodstream and does not add breast cancer or clot risk, which makes it an option for many women who cannot or prefer not to take systemic HRT [1]. Evidence grade: strong.
Bone Protection and Fewer Fractures
HRT slows the bone loss that accelerates after menopause and lowers fracture risk. The Women's Health Initiative, which followed more than 25,000 women, recorded fewer fractures in women taking hormone therapy, and this protection is why HRT is especially valued for early or surgical menopause before age 45, when years of extra bone loss would otherwise stack up [10][8][2]. Reviews of the osteoporosis literature reach the same conclusion [9][1]. Evidence grade: strong.
Possible but Unproven Benefits: Heart, Brain, Mood, and Muscle
This is where honesty matters most, because several popular claims run ahead of the evidence. A heart benefit appears possible when HRT is started early in menopause, but it is timing-dependent and is not, on its own, a reason to prescribe HRT [2][8]. Some pages claim HRT cuts Alzheimer's or dementia risk, in some cases stating it is halved; the NHS is explicit that the effect of HRT on dementia risk is unknown, so a protective effect should not be counted as a benefit [1][6]. Mood benefits appear limited to low mood that is itself driven by menopause rather than to depression in general [1]. The NHS also notes that HRT may help maintain muscle strength [1]. Evidence grade: mixed and emerging.
Cons of HRT: The Risks in Real Numbers
Most articles describe HRT risks with relative percentages, which sound alarming and tell you little. Absolute numbers, the actual extra cases per 1,000 women, are far more useful, so that is what this section uses.
Breast Cancer
Combined HRT is associated with a small increase in breast cancer risk: about 5 extra cases per 1,000 women who take it for 5 years, compared with women who do not [1]. The increase rises with longer use and with age, and it falls after you stop [7]. Estrogen-only HRT carries little or no increase in breast cancer risk, and the Cleveland Clinic frames the added combined-HRT risk as small, under 1 extra case per 1,000 women per year [3]. For the full picture, including how family history and breast density factor in, see HRT and breast cancer risk in detail.
Blood Clots and Stroke
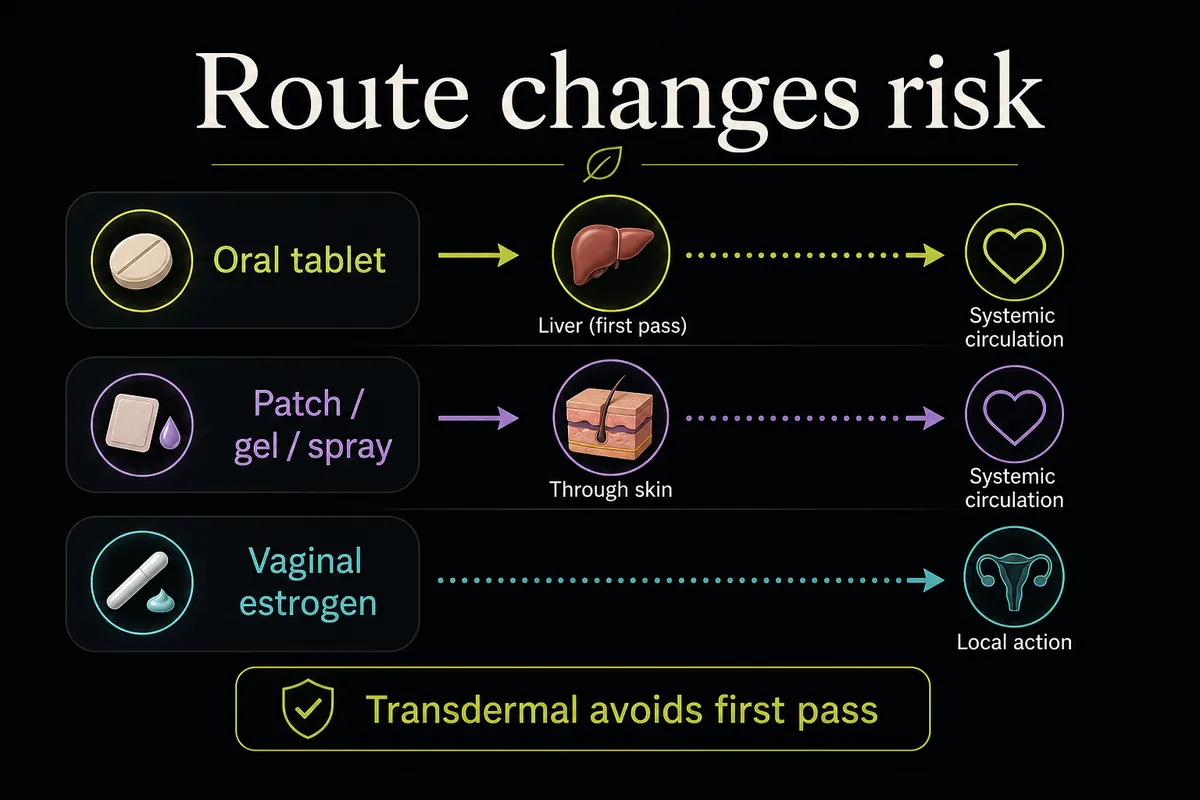
Oral HRT tablets carry a small increased risk of blood clots (venous thromboembolism). Estrogen delivered through the skin as a patch, gel, or spray does not measurably increase clot risk, because it bypasses the first-pass processing in the liver that drives the clotting effect of tablets [1][2]. Stroke risk follows a similar pattern: the increase is small, is seen mainly with oral forms, and rises with age [1]. For most women, choosing a transdermal route is the simplest way to take the clot and stroke concerns off the table.
Endometrial Cancer
Estrogen taken on its own stimulates the lining of the uterus and, over time, raises the risk of endometrial cancer, but this risk applies only to women with a uterus who take unopposed estrogen [4][6]. Adding a progestogen (making it combined HRT) protects the lining and removes this excess risk, which is exactly why combined HRT exists. Women who have had a hysterectomy do not need the progestogen and use estrogen-only HRT.
Side Effects vs Risks
It helps to separate side effects from risks. Side effects such as breast tenderness, bloating, and spotting are common in the first weeks and usually settle within about 3 months as your body adjusts; they are uncomfortable but not dangerous. The statistical risks above (breast cancer, clots, stroke, endometrial cancer) are a different category. For practical management of the day-to-day effects, see HRT side effects and how to manage them.
2025 regulatory update: On November 10, 2025, the FDA announced it was initiating the removal of the boxed ("black box") warnings from menopausal hormone therapy products, directing manufacturers to update labeling that had carried broad cardiovascular, breast cancer, and dementia warnings since the early 2000s [11]. The agency is keeping the boxed warning about endometrial cancer for systemic estrogen-alone products [11]. The change reflects newer evidence that the balance of risk depends heavily on age at initiation and hormone type; it does not erase the risks described above, and every decision remains individual.
How Age and Timing Change the Balance
More than any other factor, when you start HRT decides whether the benefits outweigh the risks. The favorable window is starting before age 60 or within 10 years of your last period; in that window, symptom relief and bone protection generally outweigh the small risks for women without contraindications [1][5]. Starting HRT for the first time well after 60 raises the cardiovascular and clot considerations, which is one reason the older average age of participants in the original Women's Health Initiative trial, around 63, made its early results look worse than they are for younger women starting near menopause [8].
Early and premature menopause is the mirror image. If menopause happens before 45, whether naturally or after surgery, HRT is actively recommended to protect the bones and heart until roughly the natural age of menopause, rather than being something to weigh cautiously [1][5]. At the other end, continuing HRT past 60 or 65 is individualized rather than an automatic stop; the decision turns on your symptoms, your risks, and your preferences with your clinician. See benefits of HRT after 65 for that specific question.
How the Type of HRT Changes the Pros and Cons
The same active hormone can carry a different risk profile depending on how it is delivered. This is the second table worth keeping, because it turns the pros and cons of HRT into practical choices you can raise with a prescriber.
| Route | Treats | Blood clot risk | Stroke risk | Notes |
|---|---|---|---|---|
| Oral tablets | Systemic symptoms: hot flashes, night sweats, mood, bone | Small increase | Small increase (age-related) | Simple to take; the route that carries the clot and stroke signal [1] |
| Transdermal patch, gel, or spray | The same systemic symptoms as tablets | No measurable increase | No measurable increase | Often preferred if you have clot risk factors; absorbed through the skin, bypassing first-pass liver metabolism [1][2] |
| Low-dose vaginal estrogen | Vaginal dryness, painful sex, urinary symptoms | No measurable increase | No measurable increase | Acts locally with minimal absorption; does not add breast cancer or clot risk [1] |
Two recaps in risk terms. First, estrogen-only versus combined: estrogen-only HRT carries little or no breast cancer increase but is only appropriate after a hysterectomy, while combined HRT adds the small breast cancer signal in exchange for protecting the uterine lining [1][7]. Second, if you have clot risk factors, a transdermal route is generally preferred over tablets because it avoids the clot and stroke signal entirely [2]. For the delivery methods in depth, see types of HRT compared and how HRT patches work.
Who Should Not Take HRT
HRT is usually advised against, and worth a careful conversation with your clinician, if you have any of the following [1][3]:
- A history of breast, ovarian, or uterine (endometrial) cancer - A prior blood clot (deep vein thrombosis or pulmonary embolism) or stroke - Active liver disease - Unexplained vaginal bleeding that has not yet been investigated - Known or suspected pregnancy
Smoking is not an automatic barrier, but it raises clot and cardiovascular risk and is worth discussing, since it can steer the choice toward a transdermal route. None of these is a blanket lifelong ban in every case; each is a reason to individualize the decision rather than to decide it in advance.
Alternatives if HRT Is Not Right for You
If HRT is not suitable or not wanted, several non-hormonal options can ease menopause symptoms [2]. On the prescription side, newer targeted medicines such as fezolinetant and elinzanetant act on the brain pathway behind hot flashes, and low-dose SSRIs or SNRIs (for example paroxetine), gabapentin, and oxybutynin are also used for vasomotor symptoms; your clinician can match one to your history. Vaginal moisturizers and lubricants help genitourinary symptoms without hormones, and lifestyle steps (sleep, layered clothing, limiting triggers, regular exercise) support the rest. Be cautious with over-the-counter supplements, which are not held to the same evidence standard and should not be assumed to work. If you are exploring non-hormonal support, see our overview of peptide support options for menopause.
How to Decide: A Simple Framework
You do not need to resolve every nuance to have a useful conversation with a prescriber. Two short checklists capture where most of the balance sits.
HRT is more likely to make sense if you:
- Are under 60 or within 10 years of your last period - Have moderate to severe hot flashes, night sweats, or genitourinary symptoms - Have no history of a hormone-sensitive cancer, blood clot, or stroke - Went through menopause early (before 45) or had your ovaries removed
The balance shifts against HRT if you:
- Are starting for the first time after age 60 - Have had breast cancer, a blood clot, or a stroke - Have active liver disease - Have unexplained vaginal bleeding that has not been checked
Where you land is a shared decision, weighing how much your symptoms affect your life against your personal risk profile, not a verdict a chart can hand down. Not sure where you fall? Our do I need HRT quiz is a structured way to check whether your symptoms and history point toward HRT. If you are ready to talk it through with a prescriber, compare the best online HRT providers to find one that fits.
Frequently Asked Questions
References
- NHS. Benefits and risks of hormone replacement therapy (HRT). NHS, 2024. https://www.nhs.uk/medicines/hormone-replacement-therapy-hrt/benefits-and-risks-of-hormone-replacement-therapy-hrt/
- Mayo Clinic Staff. Hormone therapy: Is it right for you? Mayo Clinic, 2025. https://www.mayoclinic.org/diseases-conditions/menopause/in-depth/hormone-therapy/art-20046372
- Cleveland Clinic. Hormone Therapy for Menopause Symptoms. Cleveland Clinic, 2023. https://my.clevelandclinic.org/health/treatments/15245-hormone-therapy-for-menopause-symptoms
- American College of Obstetricians and Gynecologists. Hormone Therapy for Menopause (FAQ). ACOG. https://www.acog.org/womens-health/faqs/hormone-therapy-for-menopause
- The Menopause Society. Hormone Therapy (patient education). The Menopause Society. https://menopause.org/patient-education/menopause-topics/hormone-therapy
- National Cancer Institute. Menopausal Hormone Therapy and Cancer. NCI. https://www.cancer.gov/about-cancer/causes-prevention/risk/hormones/mht-fact-sheet
- American Cancer Society. Menopausal Hormone Therapy and Cancer Risk. American Cancer Society. https://www.cancer.org/cancer/risk-prevention/medical-treatments/menopausal-hormone-replacement-therapy-and-cancer-risk.html
- Rossouw JE, et al. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women (Women's Health Initiative). JAMA, 2002. https://pubmed.ncbi.nlm.nih.gov/12117397/
- Gambacciani M, Levancini M. Hormone replacement therapy and the prevention of postmenopausal osteoporosis. Menopause Review (Prz Menopauzalny), 2014. https://doi.org/10.5114/pm.2014.44996
- Cedars-Sinai. Hormone Replacement Therapy: Is It Right for You? Cedars-Sinai, 2023. https://www.cedars-sinai.org/stories-and-insights/expert-advice/hormone-replacement-therapy-risks-benefits
- U.S. Food and Drug Administration and HHS. HHS Advances Women's Health, Removes Misleading FDA Warnings on Hormone Replacement Therapy. FDA, November 2025. https://www.fda.gov/news-events/press-announcements/hhs-advances-womens-health-removes-misleading-fda-warnings-hormone-replacement-therapy
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.