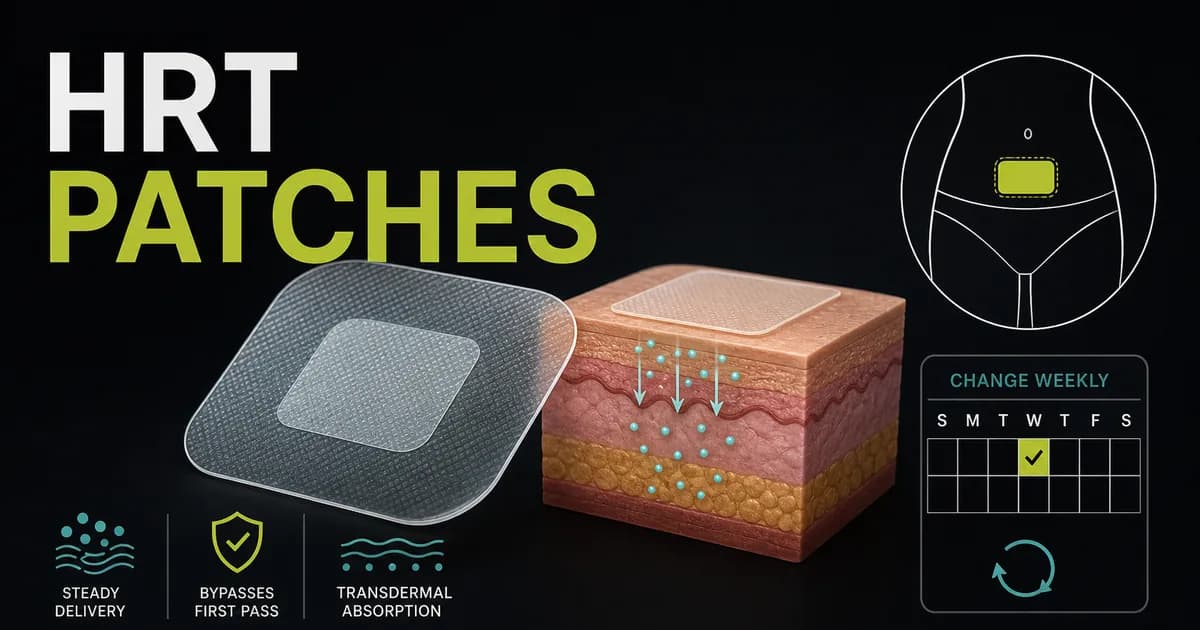
HRT patches are small adhesive squares that release estradiol, a form of estrogen, through your skin and into your bloodstream to treat menopause symptoms like hot flashes and night sweats. This guide explains how HRT patches work, exactly where to put them, which US brands and generic names exist, the side effects to watch for, and how patches compare with gels and pills in one side-by-side table. We also answer a question almost no other page covers well, whether you still have periods on patches, and note the 2026 estrogen patch supply squeeze that has some women switching brands or routes with their prescriber.
| Quick fact | What it means |
|---|---|
| Delivers estradiol through the skin | Steady release into the bloodstream, no daily pill peaks [4] |
| Change schedule: once or twice weekly | Depends on the brand; some are weekly, some are changed twice a week [1][2] |
| Two types: estrogen-only and combined | Anyone with a uterus needs the combined type or a separate progestogen for endometrial protection [6] |
| Bypasses the liver | Linked to a lower blood clot risk than oral estrogen in observational studies [8][9] |
🔑 Key Takeaways
- HRT patches deliver estradiol transdermally, giving steadier hormone levels than a daily tablet, which peaks and dips [4][7].
- Placement is below the waist, on the lower abdomen or upper buttock, never on or near the breasts [2][4].
- Estrogen-only vs combined matters. If you still have a uterus you need a progestogen alongside the estrogen to protect the womb lining [6].
- The clot-risk signal is lower than pills. Because the patch skips first-pass liver metabolism, observational studies link it to lower blood clot risk than oral estrogen, though the right choice depends on your personal history [8][9].
- Brands differ mostly in adhesive and schedule, not the hormone. If one patch irritates your skin, a different brand often solves it [1][2].
What Are HRT Patches and How Do They Work?
An HRT patch is a transdermal delivery system: estradiol is held in the patch and absorbed steadily through the skin into the bloodstream over several days [4]. That steady release is the main difference from a daily HRT tablet, which produces a peak after you swallow it and a trough before the next dose. A patch keeps the level flatter, which many women find easier on symptoms and side effects [7].
There are two physical designs. A matrix patch holds the estradiol dissolved in the adhesive layer, so the drug is spread through the whole patch, while a reservoir patch holds it in a small fluid compartment behind a rate-controlling membrane. Most modern patches are the thinner matrix type; the original Estraderm is a reservoir design. Both work equally well; the practical difference is feel and adhesion.
The HRT estrogen patch comes in two clinical types. An estrogen-only patch delivers estradiol alone and is used by women who have had a hysterectomy. A combined patch delivers estradiol plus a progestogen. Anyone who still has a uterus needs a progestogen, either built into a combined patch or taken separately, because estrogen on its own thickens the womb lining and raises the risk of endometrial cancer over time; the progestogen protects that lining [6].
The liver point is why many clinicians reach for a patch. Swallowed estrogen passes through the liver first, which raises the production of clotting factors; a patch bypasses that first-pass step. The extra clot risk from oral estrogen is small for most healthy women, but observational studies consistently link the transdermal route to a lower blood clot risk, which is why patches are often preferred for women who carry extra clot risk [8][9]. For the wider picture, see our full guide to HRT for women. HRT patches for menopause treat the same core symptoms as any systemic HRT: hot flashes, night sweats, sleep disruption, and mood and genitourinary symptoms.
HRT Patches Brands: US Brand and Generic Names
Most HRT patches on the US market are the same active ingredient, estradiol, packaged by different manufacturers. They differ in patch size, adhesive, available strengths, and whether they are changed once or twice a week. The table below separates estrogen-only patches from combined patches and notes generic availability. The change frequencies shown reflect each product's standard US labeling [1][2].
| Brand | Hormones | Type | How often changed | Generic available |
|---|---|---|---|---|
| Alora | Estradiol | Estrogen-only | Twice weekly | Yes, as estradiol transdermal system |
| Climara | Estradiol | Estrogen-only | Once weekly | Yes |
| Menostar | Estradiol (low dose) | Estrogen-only | Once weekly | Limited |
| Minivelle | Estradiol | Estrogen-only | Twice weekly | Yes |
| Vivelle-Dot | Estradiol | Estrogen-only | Twice weekly | Yes |
| Dotti | Estradiol | Estrogen-only | Twice weekly | Authorized generic of Vivelle-Dot |
| Lyllana | Estradiol | Estrogen-only | Twice weekly | Estradiol transdermal system |
| Estraderm | Estradiol (reservoir) | Estrogen-only | Twice weekly | Limited |
| CombiPatch | Estradiol + norethindrone acetate | Combined | Twice weekly [5] | Limited |
| Climara Pro | Estradiol + levonorgestrel | Combined | Once weekly [11] | Limited |
| Generic estradiol transdermal system | Estradiol | Estrogen-only | Once or twice weekly by product | This is the generic |
Sources: Mayo Clinic brand list [1], Cleveland Clinic brand list [2], CombiPatch FDA label [5], and the Climara Pro prescribing information [11]. As a rule, twice-weekly patches such as Alora, Minivelle, and Vivelle-Dot are changed every 3 to 4 days, while once-weekly patches such as Climara, Menostar, and Climara Pro are changed every 7 days [1][2].
When people search for the best HRT patches reviews, they usually hope one brand is clinically superior. The honest answer is that they all deliver estradiol, so on symptom relief they are broadly equivalent at matched doses. They differ in practical ways: adhesive strength, patch size, available strengths, and change schedule. That is why we do not publish star ratings or testimonials here; there is no verified head-to-head data crowning one estradiol patch "the best." The real decision driver is tolerance. If one brand's adhesive leaves your skin red or the patch peels, a different brand often fixes it, which is the most useful thing to know when choosing between them [1][2]. For dose context across strengths, see our HRT dosage chart.
Where to Put HRT Patch: Best Location and Placement
The best place to put an HRT patch is on the lower abdomen, below the waistline, or on the upper buttock. Many labels also allow the hip or upper outer thigh, so check your specific brand's instructions [1][2]. The skin should be clean, dry, cool, hairless, and intact. Rotate the site each change so you are not applying to the same skin twice in a row, which reduces irritation [2].
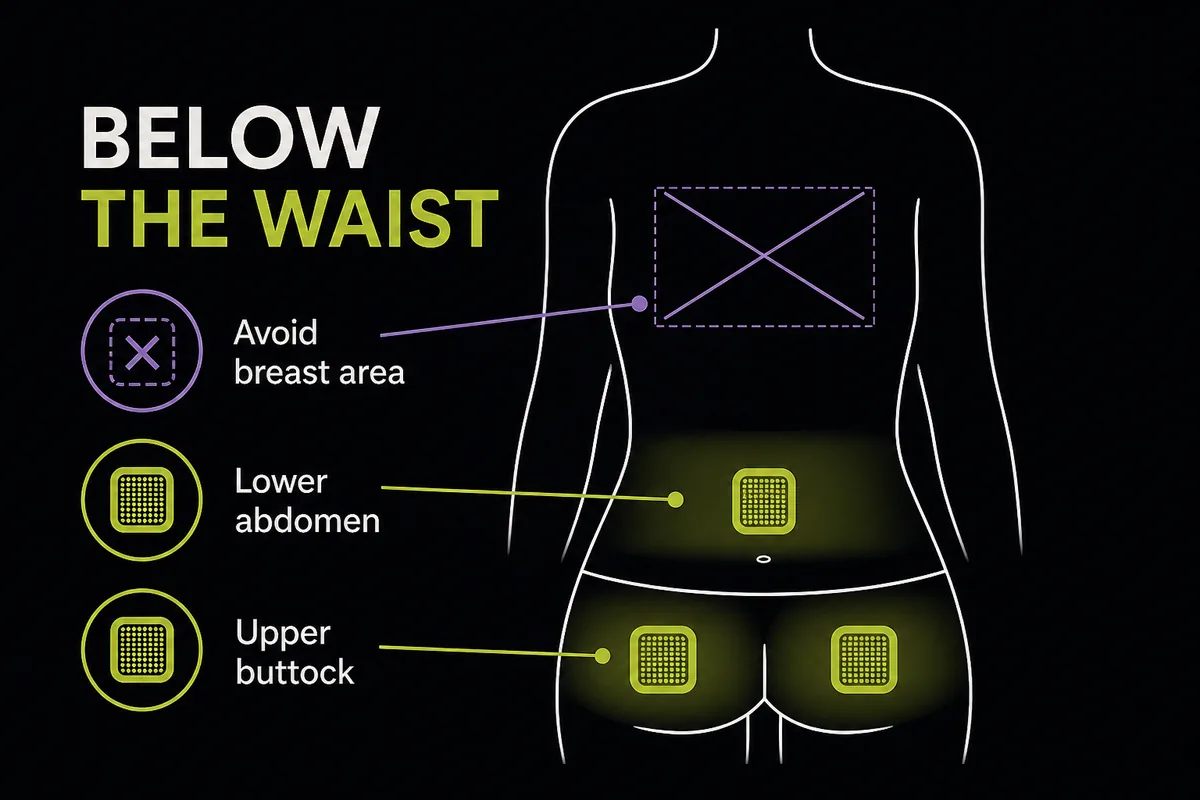
Sites to avoid: the breasts or anywhere near them, the waistband and any spot where a belt or tight clothing rubs, oily, broken, cut, or irritated skin, skin folds, freshly moisturized skin, and areas that get a lot of direct sun. Do not put lotion, oil, or powder on the skin under the patch, because it stops the patch sticking and can affect absorption [2][4].
A simple six-step application routine covers where to place an HRT patch and how to make it stay:
1. Choose a clean, dry, hairless spot below the waist, and pick a different site than last time. 2. Wait until the skin is fully dry and cool. Do not apply right after a hot shower or exercise. 3. Open the pouch and peel off half the protective backing without touching the sticky surface. 4. Press the exposed adhesive onto the skin, then peel away the rest of the backing. 5. Smooth the whole patch down flat with your palm and press firmly for about 10 seconds, running a finger around the edges. 6. Note your change day. Fold used patches in half, sticky sides together, and discard out of reach of children and pets [2].
Why Do HRT Patches Have to Be Below the Waist?
Two reasons, and no page in the search results actually explains them. First, patches are kept off and away from the breasts because the goal is systemic estradiol through the general circulation, not concentrated estrogen exposure to breast tissue; product labeling specifically instructs users not to apply to or near the breasts [2][4]. Second, the lower abdomen and buttock are practical: they have reliable, well-studied absorption, they sit below the waistband friction zone so the patch is less likely to peel, and the skin there is less exposed to sun and daily abrasion than the arms or upper body. So "below the waist" is partly a safety instruction about the breasts and partly about keeping the patch on and absorbing evenly.
How to Stop HRT Patches Falling Off
Adhesion problems are the most common patch complaint, and most are fixable. Apply only to fully dry, cooled skin, and press firmly for a full 10 seconds. Avoid lotions, oils, and powders on the site, since they undermine the adhesive, and let the skin cool after a shower or workout before reapplying, because heat and sweat loosen patches. If an edge lifts, you can sometimes secure it with skin-safe medical tape, but ask your pharmacist which tape is appropriate rather than using household tape. If a patch falls off completely, try pressing the same one back on; if it will not stick, apply a fresh patch to a different site and keep your original change days [2][4].
HRT Patch Side Effects
The most common HRT patch side effects are mild and often settle within the first few months. At the application site you may see redness, itching, or irritation. More generally, some women get headaches, breast tenderness, nausea, bloating, or light spotting as the body adjusts [4]. Skin reactions are frequently brand-specific, which is worth repeating: an irritation from one patch's adhesive often disappears when you switch to another brand [2].
Serious side effects are uncommon but real, and they mirror the risks of systemic HRT generally: blood clots, stroke, and a small change in the risk of certain cancers, all weighed against your personal history [6]. It helps to see these in absolute terms. For most healthy women in their 50s starting HRT, the added risk of any single serious event is small, on the order of a handful of extra cases per 1,000 women over several years, and it varies with age, dose, duration, and hormones used [6]. The route matters: because it bypasses the liver, observational studies link estrogen patches to a lower blood clot risk than oral estrogen, though this is an observational signal rather than proof [8][9].
Call your clinician promptly for warning signs that are never "just adjustment": swelling, pain, or warmth in one leg, sudden chest pain or breathlessness, sudden severe headache or vision change, or any unusual or heavy vaginal bleeding. For the full picture across every delivery method, read HRT side effects across all forms.
Which Is Better HRT Patches or Gel?
There is no single winner between patches and gel; they suit different people. Both are transdermal estradiol, so both bypass the liver and carry the same lower clot-risk signal versus oral estrogen [7][9]. The difference is how you live with them. A patch is set-and-forget: apply it once or twice a week and the dose stays fixed and steady. A gel is applied daily, which lets you fine-tune the dose with your prescriber and avoids adhesive skin reactions, but you have to remember it every day, wait for it to dry, and avoid skin-to-skin transfer until it absorbs [4]. If patches keep irritating your skin or will not stay on, gel is the natural alternative; if you would rather not think about your HRT daily, a patch wins.
Changing From HRT Patches to Gel
People switch from patches to gel for a few practical reasons: adhesive irritation, patches that will not stick in heat or humidity, or availability during a shortage. Dose equivalence between a patch and gel is not something to work out yourself, because the products are dosed differently; your clinician converts the dose. The switch is usually timed to a patch-change day so there is no gap in coverage. In short, changing from HRT patches to gel is a straightforward, common move, but it is a clinician-managed one, not a swap to improvise at home.
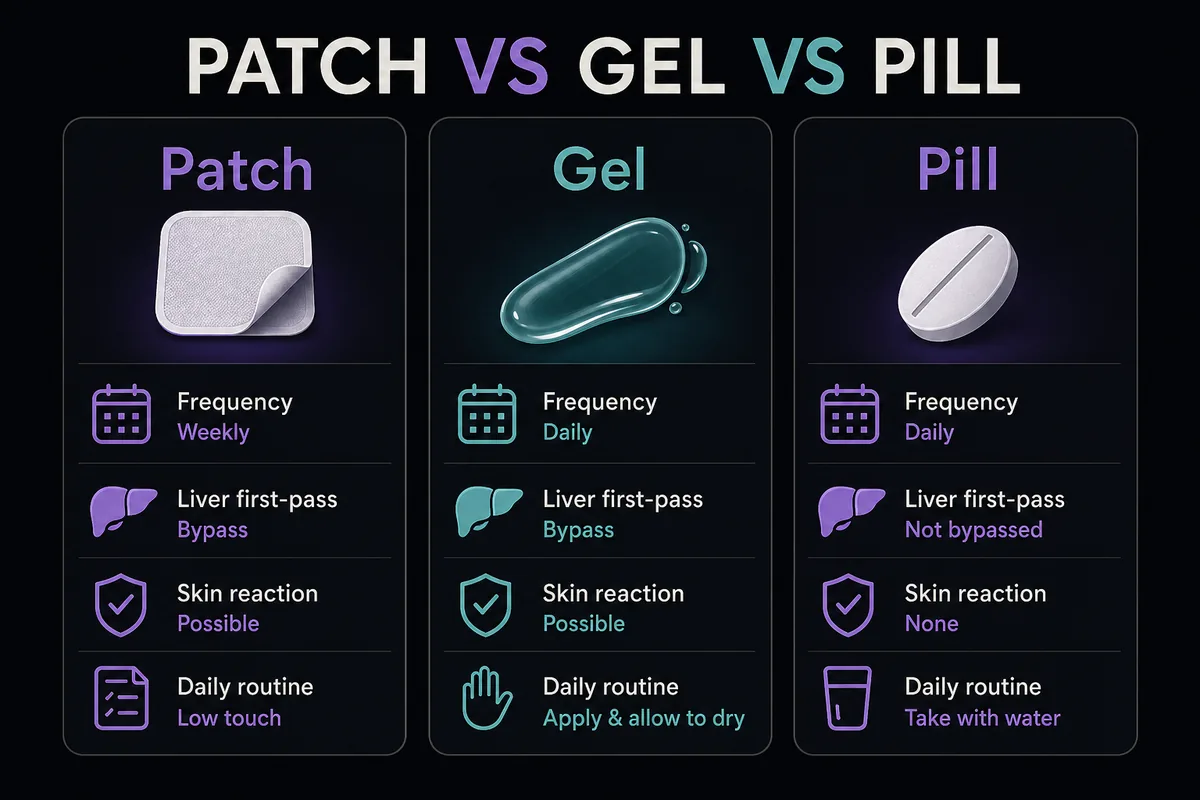
HRT Patch vs Pill vs Gel: Comparison Table
No other page in the search results compares all three routes in one place, so here is the full side-by-side. This is the patch decision viewed against its two main alternatives.
| Feature | Patch | Gel | Pill |
|---|---|---|---|
| How it is taken | Adhesive worn on the skin | Gel rubbed onto the skin | Tablet swallowed |
| Dosing frequency | Once or twice weekly | Daily | Daily |
| Liver first-pass | Bypassed (transdermal) | Bypassed (transdermal) | Passes through the liver first [9] |
| Blood clot risk signal | Lower vs oral in observational studies [8][9] | Lower vs oral in observational studies [8][9] | Reference (higher relative signal) [9] |
| Skin reactions | Possible adhesive or site irritation | Possible mild irritation, no adhesive | None |
| Daily routine burden | Low, change 1 to 2 times a week | Daily application and dry time | Daily tablet |
| Good fit for | Steady levels, set-and-forget, extra clot-risk factors | Dose flexibility, adhesive intolerance | Those who prefer a tablet, low clot risk, want cheap generics |
The patch has three advantages over the pill: no first-pass liver metabolism and therefore a lower clot-risk signal, steady multi-day levels instead of daily peaks and troughs, and no daily dose to remember [7][9]. The pill has its own advantages: no skin to react to, and it is widely available as inexpensive generics, which matters for cost. Gel sits between them, transdermal like the patch but dosed daily like the pill. For the whole HRT landscape beyond these three, see all types of HRT compared.
Do You Still Have Periods on HRT Patches?
Whether you still have periods on HRT patches depends on your regimen, not on the patch itself. There are three common scenarios. On sequential (cyclical) combined HRT, where the progestogen is taken for part of each cycle, you usually get a monthly withdrawal bleed similar to a light period; this is expected and is the regimen most perimenopausal women start on. On continuous combined HRT, where estrogen and progestogen are taken together every day, the aim is no monthly bleed once you are past the adjustment window; this is the usual postmenopausal regimen. And on an estrogen-only patch, used after a hysterectomy, there is no womb lining to shed, so there is no bleed [3][6]. So the patch does not decide your bleeding pattern; your hormone regimen does.
How to Stop Bleeding on HRT Patches
Some spotting or breakthrough bleeding is common in the first three to six months on any new HRT regimen while your body adjusts, and it usually settles on its own [3]. Missed or late patch changes are a frequent, avoidable trigger, so keeping to your schedule often reduces it. Bleeding that needs review rather than watchful waiting includes new bleeding after a stretch with none, bleeding that is heavy, or bleeding that persists beyond the first several months. For the full picture of causes and when to act, see our dedicated guide to bleeding on HRT: causes and when to see a doctor.
How Long Do HRT Patches Take to Work and What to Expect
An HRT patch reaches steady estradiol levels within a few days of your first application [4]. Symptom relief follows a rough sequence: hot flashes and night sweats often ease within a few weeks, sleep and mood tend to improve over the first month or two, and most people reach the fuller benefit by around three months, which is also when clinicians typically schedule a dose review. When people search for before and after HRT patches, they are looking for a realistic sense of change, so here it is honestly: expect gradually fewer and milder flashes, better sleep, and steadier mood over weeks to months, not an overnight transformation. We do not publish before-and-after photos or invented testimonials. For the full ramp-up across all HRT forms, see how long HRT takes to work.
Can You Smoke on HRT Patches?
Smoking raises the risk of blood clots and stroke on estrogen therapy, and that risk climbs with age, particularly over 35 [2]. Using a patch instead of a pill does not remove this risk, because smoking affects the cardiovascular system regardless of how the estrogen is delivered. Smoking also tends to make hot flashes worse, so it can work against the very symptoms you are treating. This is a conversation to have openly with your prescriber, who will factor your smoking status into the decision about whether, and how, to prescribe HRT; it is not a reason to hide it.
Who Should Not Use HRT Patches
HRT patches are not suitable for everyone. Situations that usually rule out estrogen patches, or call for careful specialist review, include a history of breast cancer or endometrial cancer, unexplained vaginal bleeding that has not been investigated, a history of blood clots (deep vein thrombosis or pulmonary embolism), a recent heart attack or stroke, active liver disease, and pregnancy [2][4]. Your prescriber will go through your full history before starting.
Some medicines interact with estradiol. The list below is not exhaustive, so tell your prescriber and pharmacist about everything you take:
- Carbamazepine, phenytoin, and other enzyme-inducing anticonvulsants - Rifampin and rifabutin - Some antifungals such as ketoconazole and itraconazole - HIV medicines such as ritonavir - St John's wort - Levothyroxine, where estrogen can change thyroid hormone requirements and timing
Your clinician manages these interactions; do not start or stop anything on your own [4].
The 2026 Estrogen Patch Shortage: What to Know
US supply of some estrogen patches tightened in 2026, and the FDA has been involved in tracking and addressing the disruption, according to reporting by USA Today [10]. If your usual patch is hard to find, do not ration doses or improvise. The options people typically discuss with their prescriber include switching to a different patch brand of the same estradiol, moving to a gel, or considering another route, all of which are clinician-managed decisions rather than DIY swaps [10]. Availability can also raise cost questions when you change brand or route, so it is worth reading what HRT costs with and without insurance before you call the pharmacy. We are not promising any particular brand is in stock or quoting prices here, because both change quickly.
Frequently Asked Questions
If you are looking to start or switch HRT patches, online HRT services that prescribe patches can connect you with a clinician, and our guide to what HRT costs with and without insurance covers the price side. If you are also exploring non-hormonal support, see our overview of peptides for menopause symptoms.
References
- Mayo Clinic. Estradiol (transdermal route): description and brand names. Accessed 2026. https://www.mayoclinic.org/drugs-supplements/estradiol-transdermal-route/description/drg-20075306
- Cleveland Clinic. Estradiol Skin Patches. Accessed 2026. https://my.clevelandclinic.org/health/drugs/18198-estradiol-skin-patches
- NHS. Hormone replacement therapy (HRT). Accessed 2026. https://www.nhs.uk/medicines/hormone-replacement-therapy-hrt/
- MedlinePlus. Estradiol Transdermal Patch. Accessed 2026. https://medlineplus.gov/druginfo/meds/a605042.html
- US Food and Drug Administration. CombiPatch (estradiol/norethindrone acetate transdermal system) prescribing information, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/020870s033lbl.pdf
- National Cancer Institute. Menopausal Hormone Therapy and Cancer fact sheet. Accessed 2026. https://www.cancer.gov/about-cancer/causes-prevention/risk/hormones/mht-fact-sheet
- Goodman MP. Does the route of administration for estrogen matter? Menopause, 2011;18(10):1032-1033. https://journals.lww.com/menopausejournal/abstract/2011/10000/does_the_route_of_administration_for_estrogen.6.aspx
- Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of venous thromboembolism. PMC7475284. https://pmc.ncbi.nlm.nih.gov/articles/PMC7475284/
- Canonico M, Plu-Bureau G, Scarabin PY. Transdermal versus oral estrogen and risk of venous thromboembolism and gallbladder disease. PMC2500203. https://pmc.ncbi.nlm.nih.gov/articles/PMC2500203/
- USA Today. Estrogen patch shortage and the FDA response, April 17, 2026. https://www.usatoday.com/story/life/health-wellness/2026/04/17/estrogen-shortage-menopause-perimenopause-fda/89623900007/
- DailyMed. Climara Pro (estradiol/levonorgestrel transdermal system) prescribing information. Accessed 2026. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=184d3092-7fc6-4375-816b-1ab06bb99cfd
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.