HRT and breast cancer is one of the most searched and most misunderstood questions in menopause care, so here is the honest, guideline-anchored bottom line: for most women without a personal history of breast cancer, the extra risk from hormone replacement therapy is small, and it depends heavily on the type of HRT and how long it is used. Estrogen-only, combined estrogen-plus-progestogen, and low-dose vaginal HRT carry very different risk profiles. Two recent developments have kept this topic in the news: the FDA removed the long-standing "black box" warning from menopause hormone products in November 2025 [9], and a September 2025 expert consensus published in the journal Menopause reframed hormone therapy after breast cancer as an individualized decision [1]. This page explains the numbers in plain absolute-risk terms, without scaremongering, so you can discuss the specifics with your own clinician.
🔑 Key Takeaways
- HRT does not "cause" breast cancer the way a carcinogen does. Combined HRT is linked to a small increase in risk with longer use, while estrogen-only HRT is neutral to slightly protective in women without a uterus [3][4].
- The absolute increase is small. The Women's Health Initiative (WHI) found about 3 extra invasive breast cancers per 1,000 women aged 50 to 59 who take combined HRT for 5 years, which works out to fewer than one extra case per 1,000 women per year of use [4].
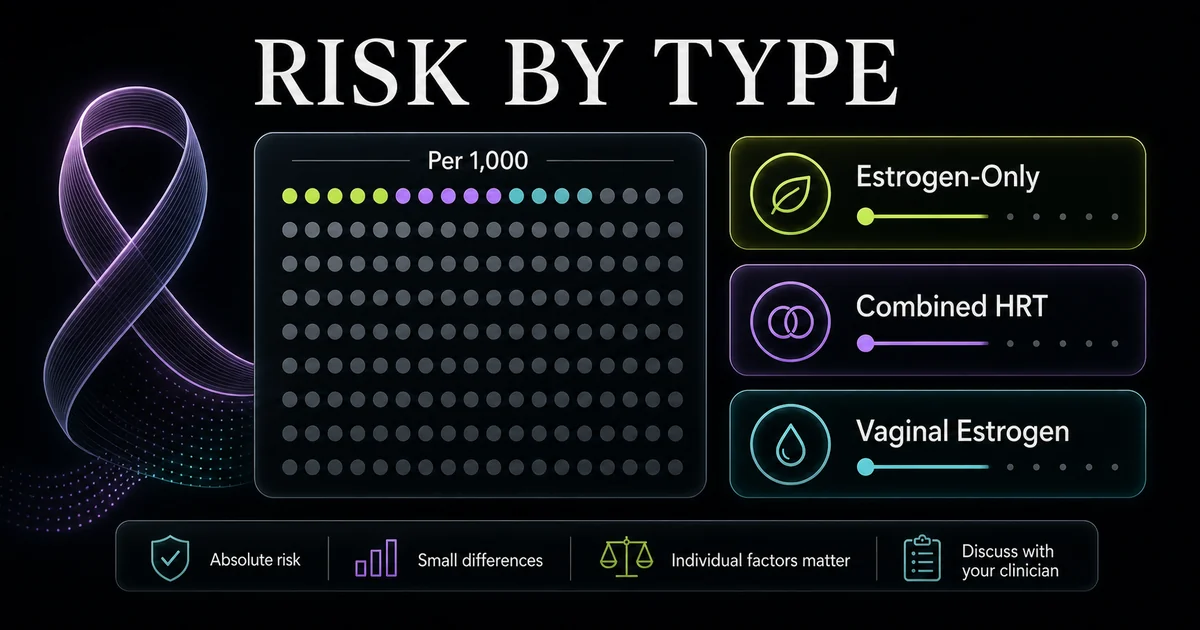
- Type matters most. Vaginal (local) estrogen carries the lowest risk, estrogen-only systemic HRT is lower risk than combined, and combined HRT carries the small increase that grows with duration [1][7].
- After breast cancer, systemic HRT is generally not recommended, especially for hormone-receptor-positive (HR+) disease, though a 2025 expert consensus supports an individualized, shared decision for some survivors after non-hormonal options fail [1].
- There are effective non-hormonal alternatives, including newer prescription medicines, low-dose vaginal estrogen for local symptoms, and lifestyle changes [3][4].
- HRT is not the same as hormone therapy for breast cancer. They are opposites: HRT replaces hormones, while endocrine therapy blocks or lowers estrogen to treat cancer [2].
Quick Stats
| Value | What it means |
|---|---|
| ~3 extra cases per 1,000 | Additional invasive breast cancers in women aged 50 to 59 on combined HRT for 5 years (WHI) [4] |
| Neutral to lower | Estrogen-only HRT effect on breast cancer risk in the WHI long-term follow-up [3][4] |
| No meaningful increase | Low-dose vaginal estrogen effect on breast cancer risk [1] |
| ~80% higher recurrence | Reported for HR+ survivors on systemic HRT in a 2021 4-study analysis [1] |
| November 2025 | FDA removed the "black box" warning from menopause hormone products [9] |
Does HRT cause cancer?
The direct answer is that HRT does not "cause" cancer the way tobacco or asbestos does. Certain types of HRT, mainly combined estrogen-plus-progestogen taken for several years, are associated with a small increase in breast cancer risk, while estrogen-only HRT is neutral to slightly protective in women without a uterus [3][4]. So the popular claim that "HRT causes cancer" is too blunt to be accurate. The more precise statement is that some forms of HRT modestly raise the risk of one cancer while leaving or lowering the risk of others.
It helps to separate association from causation. Large studies show a statistical link between combined HRT and breast cancer, but a link is not the same as a direct cause, and the size of any effect depends on several factors: the type of HRT, the dose, how long it is used, the age at which it is started, and personal or family history [3][6]. Why does HRT appear to raise breast cancer risk at all? The leading explanation is that added hormones, particularly the progestogen component of combined therapy, can stimulate the growth of hormone-sensitive breast tissue over time [4][7]. That is a mechanism of promotion in already-susceptible cells, not the creation of cancer from nothing.
The evidence base here is anchored by two landmark bodies of work. The WHI randomized trials, with their long-term follow-up, remain the reference point for absolute-risk numbers in US practice [4]. The 2019 Lancet meta-analysis from the Collaborative Group on Hormonal Factors in Breast Cancer pooled worldwide data and confirmed that risk rises with longer duration and differs by HRT type [7]. Both are covered in the sections below.
What is HRT, and which types affect breast cancer risk?
HRT (hormone replacement therapy) replaces the estrogen, and often progesterone, that the body makes less of around menopause, to relieve symptoms such as hot flashes, night sweats, and vaginal dryness. Not every form carries the same breast cancer signal, which is why understanding the main types of HRT is the single most useful thing you can do before weighing risk.
Estrogen-only HRT (for women after hysterectomy)
Estrogen-only HRT is prescribed for women who no longer have a uterus, typically after a hysterectomy. In the WHI long-term follow-up, estrogen-alone therapy was associated with a neutral to slightly lower breast cancer risk rather than a higher one [3][4]. The important caveat is that estrogen-only HRT is not appropriate if you still have a uterus, because unopposed estrogen raises the risk of endometrial (uterine) cancer. That is precisely why a progestogen is added for women with a uterus, which brings us to the type that carries the small breast cancer signal.
Combined HRT (estrogen plus progestogen)
Combined HRT pairs estrogen with a progestogen to protect the uterine lining, and it is the type most associated with a small increase in breast cancer risk [4][7]. It comes in two schedules: sequential (estrogen every day with a progestogen for part of each month, often used in perimenopause) and continuous (both hormones every day, more common after menopause). Across studies, continuous combined regimens tend to show a slightly larger association than sequential ones, and in every case a higher dose and a longer duration of use raise the risk more [5][7]. Duration is the lever that matters most: short-term use for symptom control sits at the low end of the range.
Vaginal (local) estrogen
Low-dose vaginal estrogen, delivered as a cream, ring, or tablet, treats local symptoms such as dryness and painful sex. Because very little is absorbed into the bloodstream, it is not linked to a higher breast cancer risk and is generally considered safe, including for many breast cancer survivors, based on ACOG guidance and 2023 JAMA Oncology data summarized by breast cancer nonprofits [1]. It is a fundamentally different exposure from systemic pills, patches, or gels. For how the systemic delivery routes differ, see our guide to HRT patches.
HRT breast cancer risk chart: absolute numbers by type
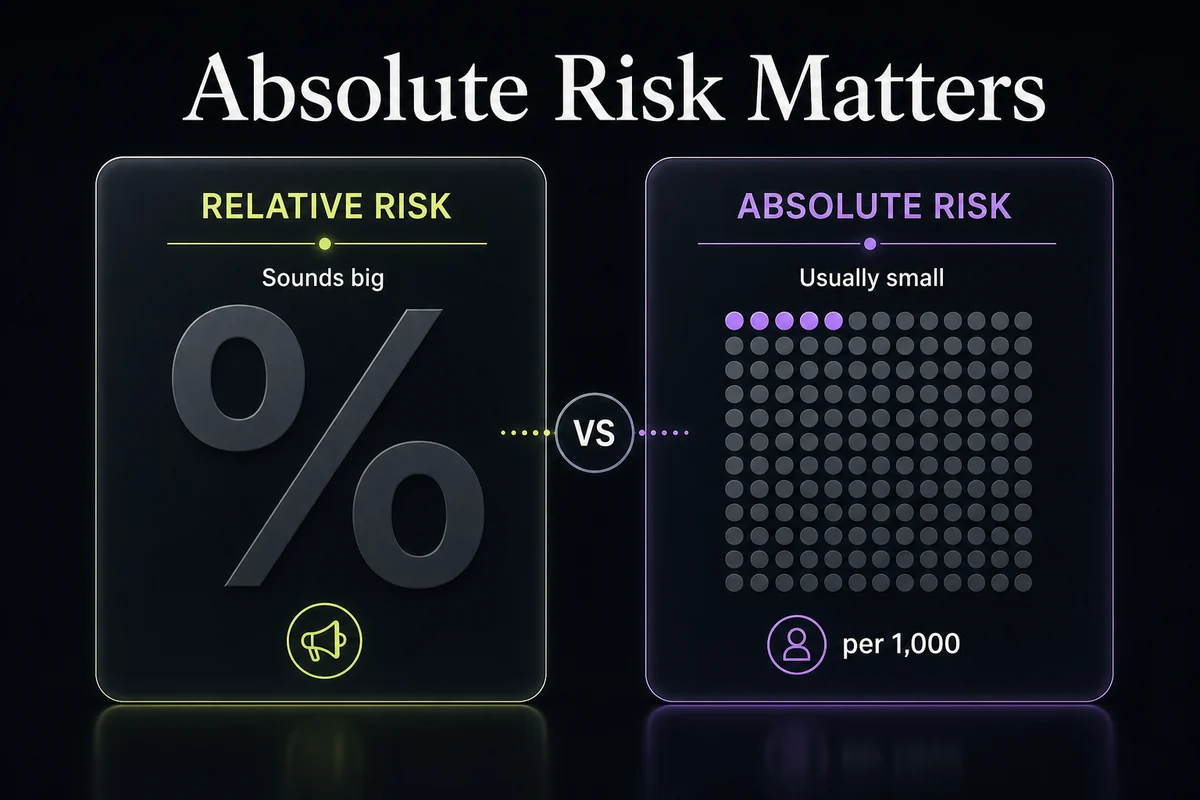
Most consumer pages describe HRT breast cancer risk in vague relative terms and never put absolute numbers in a table. The chart below does, because absolute risk is what actually tells you how likely something is. Read it alongside the plain-language explainer underneath.
HRT breast cancer risk chart (absolute risk by type and duration)
| HRT type | How it is taken | Effect on breast cancer risk | Approx. extra (or fewer) cases per 1,000 women (age 50 to 59, over 5 years) | Best for |
|---|---|---|---|---|
| No HRT (baseline) | Not applicable | Reference point | About 23 per 1,000 (baseline 5-year incidence for women aged 50 to 59) [5] | Not applicable |
| Estrogen-only HRT | Pill, patch, or gel | Neutral to slightly lower | Neutral, to about 4 fewer per 1,000, in the WHI follow-up and UK data [3][4][5] | Women after hysterectomy |
| Combined HRT, sequential | Estrogen daily plus progestogen part of each month | Small increase, grows with duration | A small number of extra cases per 1,000, fewer than continuous combined [5][7] | Perimenopause, uterus intact |
| Combined HRT, continuous | Estrogen plus progestogen daily | Small increase, larger than sequential and grows with duration | About 3 to 4 extra per 1,000 for women aged 50 to 59 over 5 years, rising with longer use [4][5] | Postmenopause, uterus intact |
| Vaginal (local) estrogen | Cream, ring, or tablet | No meaningful increase | About 0 per 1,000 [1] | Vaginal and genitourinary symptoms only |
*All figures are absolute risk for women aged 50 to 59 over about 5 years of use, and they vary by age at start, dose, and duration; the risk rises the longer HRT is used. Over a longer horizon, the 2019 Lancet meta-analysis estimated that 5 years of use starting at age 50 adds roughly 1 extra breast cancer per 50 users of continuous combined HRT, about 1 per 70 users of sequential combined HRT, and about 1 per 200 users of estrogen-only HRT, counted across ages 50 to 69 [7]. Figures are drawn from the WHI [4], the British Menopause Society Fast Facts (September 2025) [5], NICE NG23 [6], and the 2019 Lancet meta-analysis [7].*
Absolute risk vs relative risk, explained
Here is the concept nearly every headline gets wrong. When the WHI reported that combined HRT raised breast cancer risk by roughly 26 percent, that "26 percent higher" is a relative figure, and on its own it sounds alarming. In absolute terms, the same data worked out to about 3 extra invasive breast cancers per 1,000 women aged 50 to 59 who used combined HRT for 5 years [4]. A large-sounding percentage can describe a small change in the actual number of people affected. This is why clinicians frame HRT risk in cases per 1,000 rather than percentages.
Age and timing also matter. Risk is generally lower for women who start HRT between ages 50 and 59, and within about 10 years of their last period, than for those who start at 60 or older [3]. The 2019 Lancet meta-analysis and later analyses (including 2023 data) reinforced that both duration of use and the interval since menopause shape the size of the association [7]. None of this makes the decision automatic; it makes it specific to you.
Can HRT cause breast cancer to come back? HRT after breast cancer
For women with a personal history of breast cancer, the calculation changes. Systemic HRT (pills, patches, gels, or injections that circulate hormones through the body) is generally not recommended after breast cancer, especially for hormone-receptor-positive (HR+) disease, because added hormones can stimulate any remaining HR+ cells [1][4]. A 2021 analysis of four studies reported roughly 80 percent higher recurrence risk in HR+ survivors who used systemic HRT [1], and the HABITS trial in Sweden was stopped early after finding more recurrences in the HRT group [8]. That is the cautious, long-standing default in survivorship care, and it is the honest starting point for anyone asking whether HRT can make breast cancer come back.
There is an emerging nuance worth presenting fairly, and without advocacy. A September 2025 expert consensus from The Menopause Society reframes hormone therapy after breast cancer as an individualized, shared decision for a subset of survivors with severe symptoms that persist after non-hormonal options have been tried, rather than an absolute prohibition [1]. Low-dose vaginal estrogen is generally considered acceptable for local symptoms even after breast cancer, because so little is absorbed [1]. Two cautions belong here: this is a conversation to have with your oncologist, not a green light, and testosterone is not an established or safe workaround after breast cancer, so treat any source that promotes it as unreliable. The breast cancer HRT decision after a diagnosis is genuinely individual, and it belongs with your cancer team.
HRT for breast cancer survivors: what to take instead
If systemic HRT is off the table, there is still a real menu of options for breast cancer survivors, which is why "what can I take instead of HRT after breast cancer" is such a common search. The table below turns the usual wall of prose into something scannable [3][4].
| Symptom | Non-hormonal options | Notes |
|---|---|---|
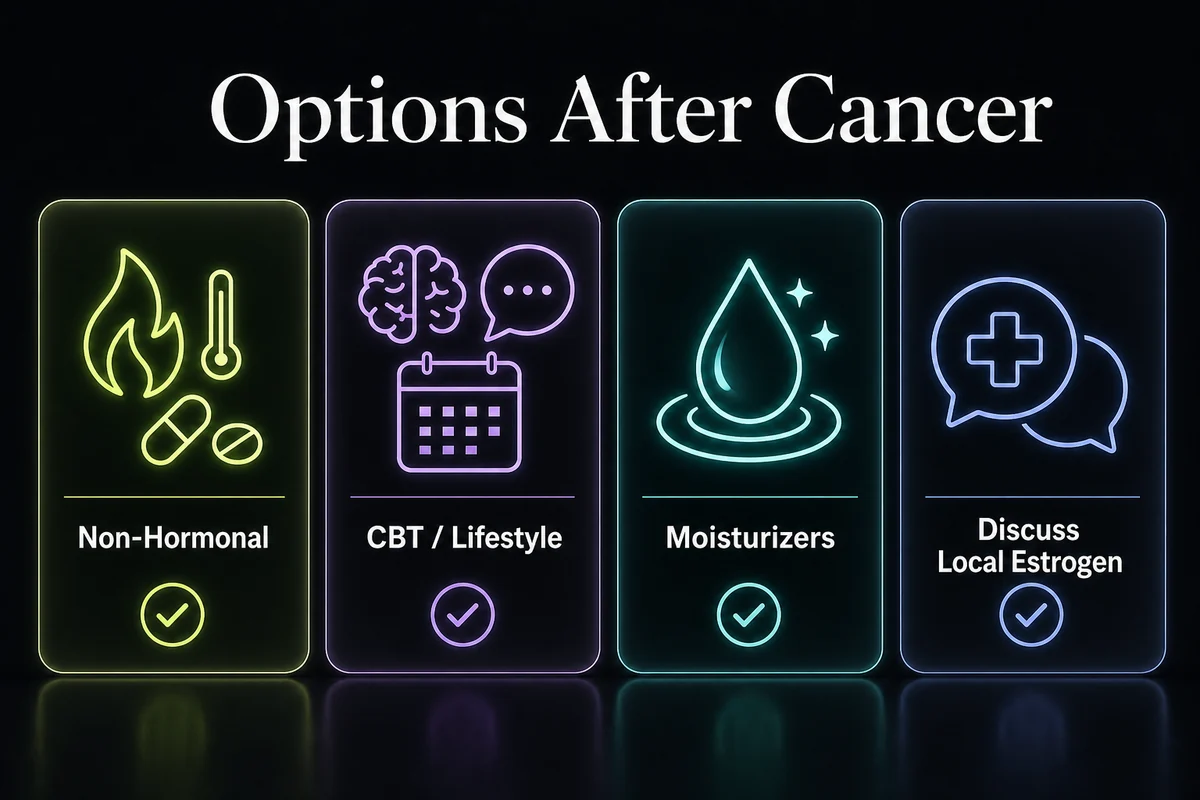
| Hot flashes and night sweats | Fezolinetant (Veozah), elinzanetant (Lynkuet), low-dose SSRIs or SNRIs, gabapentin, clonidine, oxybutynin | Newer neurokinin-targeted drugs are prescription-only; your clinician matches one to your history [3] |
| Hot flashes (non-drug) | Cognitive behavioral therapy (CBT), acupuncture, yoga, paced breathing, weight management | Evidence is strongest for CBT; others help some women [3][4] |
| Vaginal and genitourinary symptoms | Vaginal moisturizers and lubricants first; low-dose vaginal estrogen if needed | Vaginal estrogen is generally considered lower risk because little is absorbed [1] |
| General risk reduction | Maintaining a healthy weight, limiting alcohol, not smoking, regular exercise | Lifestyle factors independently influence breast cancer risk [4] |
One important interaction: if you take tamoxifen, certain antidepressants (paroxetine and fluoxetine) can interfere with how the body activates it, so a survivor on tamoxifen who needs an SSRI is usually steered toward a different one [3]. Always let your oncologist coordinate these choices. If you are exploring options beyond hormones, our overview of peptide options for menopause covers non-hormonal approaches some people ask about, and our guide to using HRT for menopause symptoms explains where hormone therapy fits for women without a cancer history.
HRT vs hormone therapy for breast cancer (they are opposites)
This distinction trips up a lot of people because the names sound alike, yet the two treatments do opposite things. HRT (hormone replacement therapy) adds estrogen, and often progesterone, to relieve menopause symptoms. Endocrine therapy for breast cancer, sometimes called hormone therapy, does the reverse: drugs like tamoxifen block estrogen's effect on breast cells, and aromatase inhibitors lower the body's estrogen, in order to treat or help prevent HR+ breast cancer [2]. So a woman can be told to avoid HRT while being prescribed "hormone therapy" for her cancer, and both statements are correct. When you read about hormone therapy, check which direction it goes: replacing estrogen or blocking it.
HRT and ovarian cancer
Beyond the breast, the most consistent additional signal in the research is a small increase in ovarian cancer risk with systemic HRT. Large pooled analyses have associated HRT use with roughly one extra ovarian cancer case per 1,000 users over about 5 years, an absolute risk that is low even though the association is real [6][10]. As with breast cancer, this is a factor to weigh rather than an automatic reason to avoid HRT, and the size of the estimate varies by study and by how long HRT is used. Ovarian cancer is far less common than breast cancer, so it usually plays a smaller role in the overall decision.
HRT and colon cancer
The picture for the colon runs the other way. In the WHI, combined estrogen-plus-progestin HRT was associated with a lower risk of colorectal cancer, while estrogen-only therapy showed no clear benefit [4]. This is a genuine finding, but it is not a reason to take HRT: guidelines do not recommend hormone therapy as a cancer-prevention strategy, and the established ways to lower colorectal cancer risk are screening and lifestyle. It is included here for balance, because "HRT and cancer" is not a one-directional story, and different cancers respond differently to the same therapy.
Can you take HRT after DCIS?
Ductal carcinoma in situ (DCIS) is a non-invasive, stage 0 breast condition, and the HRT question after DCIS is decided case by case rather than by a blanket rule. Decisions depend on the receptor status of the DCIS and the treatment you had, so systemic HRT is generally approached cautiously and only after a careful conversation with your oncologist [1]. Low-dose vaginal estrogen is often considered a lower-risk choice for local genitourinary symptoms because so little is absorbed [1]. If you have had DCIS, treat any menopause hormone decision as one to make with your cancer team, not from a general article.
How to lower your risk if you use HRT
If you and your clinician decide HRT is right for you, several practical steps keep the risk profile as favorable as possible:
- Use the lowest effective dose for the shortest duration that controls your symptoms [4][6]. - Start within about 10 years of menopause, or before age 60, which is generally the more favorable window [3]. If you are considering starting or continuing HRT after 65, the balance shifts and deserves a fresh conversation. - Ask about transdermal options (patches or gels), which some clinicians prefer for reasons beyond cancer, such as clot risk. - Keep up with mammograms, and know that combined HRT can increase breast density and lead to more callbacks, so tell the imaging center you use HRT [1]. - Bring a short list of questions to your clinician: which type and dose, for how long, how it interacts with your personal and family history, and when to reassess. This mirrors the "questions for your doctor" approach the leading cancer nonprofits recommend [1].
The cancer-risk conversation is only one part of the decision. To see the wider picture, weigh the full pros and cons of HRT, review the other HRT side effects beyond cancer, and consider the benefits many women value, including HRT and bone health and the ongoing research on HRT and dementia risk. For the complete overview, see our full guide to HRT for women.
Frequently Asked Questions
References
- Breastcancer.org. Hormone Replacement Therapy (HRT) and Breast Cancer Risk. https://www.breastcancer.org/risk/risk-factors/using-hormone-replacement-therapy
- American Cancer Society. What to Know About HRT and Cancer Risk. https://www.cancer.org/cancer/latest-news/what-to-know-about-hormone-replacement-therapy-and-cancer-risk.html
- Breast Cancer Research Foundation. HRT and Breast Cancer Risk Explained. https://www.bcrf.org/about-breast-cancer/hrt-breast-cancer-risk/
- MD Anderson Cancer Center. Does hormone replacement therapy increase cancer risk? https://www.mdanderson.org/cancerwise/does-hormone-replacement-therapy-increase-cancer-risk.h00-159699123.html
- British Menopause Society. Fast Facts: HRT and breast cancer risk. BMS, September 2025. https://thebms.org.uk/wp-content/uploads/2025/09/12-NEW-BMS-ToolsforClinicians-Fast-Facts-HRT-and-Beast-Cancer-Risk-SEPT2025-B.pdf
- NICE evidence review. HRT and breast cancer incidence and mortality. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK609657/
- Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal hormone therapy and breast cancer risk. Lancet 2019;394:1159-1168. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)31709-X/fulltext
- Holmberg L, Anderson H. HABITS (hormonal replacement therapy after breast cancer, is it safe?). Lancet 2004;363:453-455. https://doi.org/10.1016/S0140-6736(04)15493-7
- US Food and Drug Administration. FDA Approves Labeling Changes to Menopausal Hormone Therapy Products. FDA, November 2025. https://www.fda.gov/news-events/press-announcements/fda-approves-labeling-changes-menopausal-hormone-therapy-products
- Collaborative Group on Epidemiological Studies of Ovarian Cancer. Menopausal hormone use and ovarian cancer risk: individual participant meta-analysis of 52 epidemiological studies. Lancet 2015;385:1835-1842. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61687-1/fulltext
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.