HRT and osteoporosis are closely linked because the estrogen that hormone replacement therapy replaces is the main hormone that keeps bone from breaking down. After menopause, estrogen falls, bone breakdown speeds up, and bone density drops, which is why the connection between hrt and osteoporosis matters so much for women in midlife. HRT slows or stops this menopausal bone loss and lowers fracture risk, and estradiol is FDA-approved to prevent postmenopausal osteoporosis [1]. It helps to be precise about what HRT does: it prevents further loss and preserves the bone you already have rather than dramatically rebuilding a skeleton that has already thinned, and it is one option among several bone-protecting treatments. This guide explains the mechanism, the evidence, how HRT compares with bisphosphonates, the best forms and doses for bone, and who it suits.
🔑 Key Takeaways
- Estrogen protects bone, and losing it drives menopausal bone loss. Estrogen restrains the cells that break bone down, so when it falls at menopause, resorption outpaces rebuilding [2][3].
- HRT prevents osteoporosis and lowers fracture risk. Replacing estrogen preserves bone density, and estradiol is FDA-approved for prevention of postmenopausal osteoporosis [1][3].
- HRT preserves bone but does not truly reverse it. It maintains bone and produces modest density gains; anabolic drugs are what actively rebuild the skeleton [3][5].
- Timing matters most. The bone benefit is greatest for women under 60 and within 10 years of menopause, and for those with early or premature menopause [1][4].
- Protection lasts only while you take it. Bone loss can resume after stopping, which is why some women later move to a bone-specific drug [3].
| Quick fact | What it means |
|---|---|
| Estrogen restrains bone-resorbing cells through the RANKL/OPG pathway | When estrogen falls at menopause, bone breakdown accelerates [2][3] |
| Up to about 20% of bone density can be lost in the first 5 years of menopause | Bone loss is fastest early, which is why timing of treatment matters [2] |
| Estradiol is FDA-approved to prevent postmenopausal osteoporosis | HRT is a recognized prevention option, not only a symptom treatment [1] |
| A 2026 real-world study of 137,484 women linked early HRT to lower osteoporosis odds and a 13% cut in fracture risk | Fresh evidence supports early, in-window use for bone [4] |
How menopause and estrogen loss cause bone loss
Bone is living tissue in constant renewal. Two cell types keep it balanced: osteoclasts break old bone down, and osteoblasts build new bone to replace it. This cycle, called remodeling, normally stays in balance. Estrogen is one of its most important regulators, because it restrains osteoclasts, largely through a signaling system known as the RANKL/OPG pathway [3]. As long as estrogen is present, bone breakdown stays in check.
At menopause, estrogen drops sharply, the brake comes off the osteoclasts, and resorption starts to outpace formation. The result is a net loss of bone. This is why the link between osteoporosis and hrt is really a story about estrogen: put simply, the hormone HRT restores is the same one that was protecting the skeleton. Bone loss is fastest in the years right around menopause, and up to about 20% of bone density can be lost within the first 5 years [2].
Osteoporosis is often called the "silent thief" because it has no symptoms until a bone breaks, frequently at the hip, spine, or wrist [2]. Women are affected more often than men because they start with less bone mass and then go through the rapid estrogen-driven loss of menopause. Women who reach menopause early or have premature menopause lose that protection sooner and are at higher long-term risk, which is one reason clinicians pay close attention to bone in this group [2].
Does HRT prevent osteoporosis?
Yes. This is the clearest answer in the whole topic: does hrt prevent osteoporosis, and does hrt help osteoporosis? Replacing estrogen re-applies the brake on bone breakdown, preserves the bone a woman still has, and lowers fracture risk [1][3]. In the United States, the FDA-approved indication for estradiol here is specifically prevention of postmenopausal osteoporosis, which is why HRT is best thought of as a preventive and preserving option rather than the first-line drug for rebuilding an already-thin skeleton [1].
Timing shapes how much benefit you get. Guidelines describe a "window of opportunity": the bone (and overall) benefit of HRT is greatest for women who start under age 60 and within 10 years of their final period, and women with early or premature menopause tend to benefit most because they replace estrogen that was lost prematurely [1]. Starting many years after menopause, purely for bone, is a more individual decision that a clinician weighs case by case.
The evidence has continued to build. A 2026 real-world study presented at the AAOS Annual Meeting followed 137,484 postmenopausal women and found that starting HRT early after a menopause diagnosis was associated with lower odds of osteoporosis (women who did not use HRT had about 1.18 times the odds) and a 13% reduction in fracture risk at maximum follow-up [4]. On DEXA scans, bone density typically shows small gains over the first one to three years of treatment, and protection continues for as long as HRT is taken [3].
Can HRT reverse osteoporosis, and does HRT change bone structure?
The honest answer to "can hrt reverse osteoporosis" is no, not in the sense most people mean. HRT stops or slows further bone loss and can nudge bone density up modestly, but it does not dramatically rebuild a skeleton that has already thinned [3]. The right words are prevent and preserve, not reverse. Mechanistically, restoring estrogen shifts the remodeling balance back toward a small net positive, so you keep more of the bone you have and lose it more slowly [3].
That distinction matters when you compare HRT with anabolic (bone-building) drugs. Medicines such as teriparatide, abaloparatide, and romosozumab actively stimulate new bone formation and can meaningfully rebuild density in severe osteoporosis, which HRT does not do [5]. HRT belongs to the group of treatments that protect existing bone rather than the group that builds new bone.
So does hrt change bone structure, and can hrt change bone structure at the microscopic level? HRT helps maintain the internal architecture of bone. Trabecular bone, the honeycomb-like inner structure of the spine and hip, thins and develops small perforations as bone is lost after menopause. By slowing the breakdown that drives that damage, HRT helps preserve this microarchitecture and the strength that comes with it [3]. What it does not do is re-thicken and re-connect bone the way the anabolic drugs can. In short: HRT protects the structure you have; it does not remodel a weakened structure into a new one.
HRT vs bisphosphonates for osteoporosis
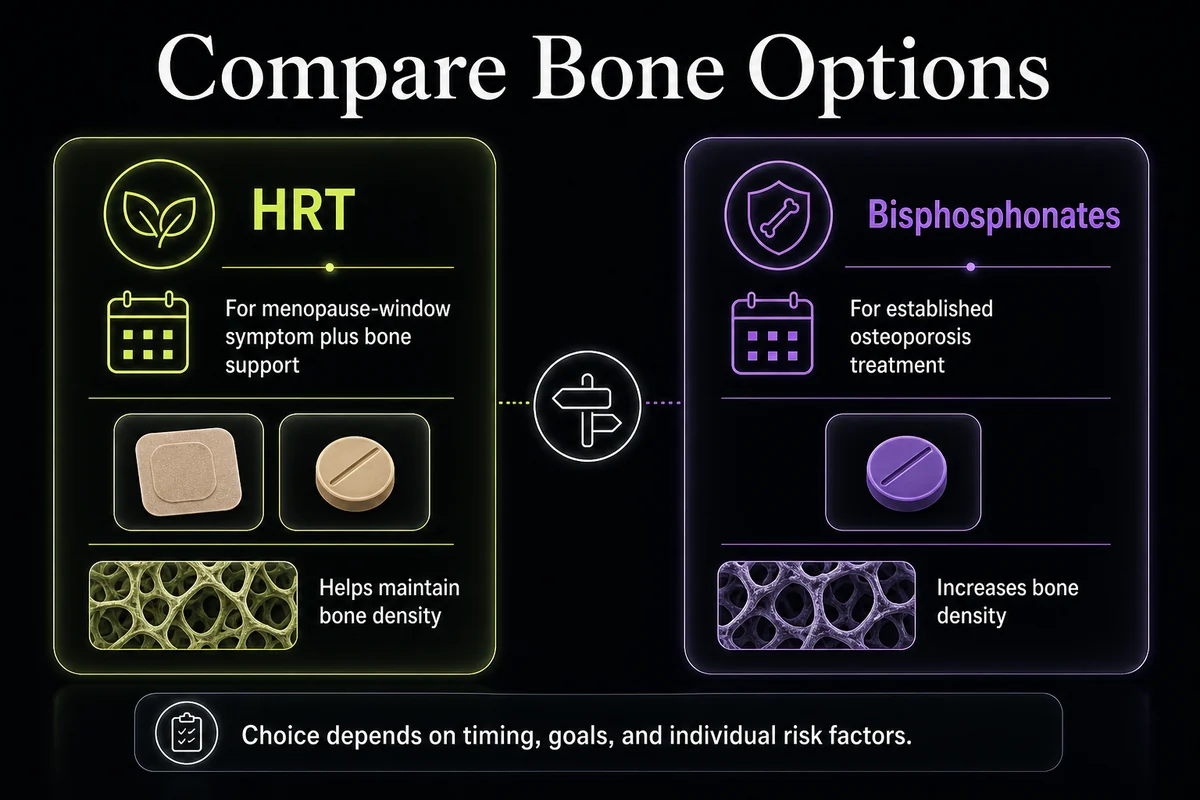
For many readers the practical question is hrt vs bisphosphonates for osteoporosis. Both slow bone breakdown, but they get there differently and suit different people. Bisphosphonates (such as alendronate, risedronate, ibandronate, and zoledronic acid) suppress osteoclasts directly and are the usual first-line drug treatment for established osteoporosis, with strong protection against vertebral, nonvertebral, and hip fractures [5]. HRT works by replacing estrogen, and guideline bodies describe it as about as effective as other osteoporosis medicines at reducing fracture risk in postmenopausal women [3]. HRT is typically chosen when a woman is early in menopause or also wants relief from menopausal symptoms, while bisphosphonates are often preferred for older women or established disease.
There is a nuance worth knowing. In the randomized WHI trial, estrogen plus progestin reduced hip and clinical vertebral fractures by roughly a third [6], but some later analyses at standard doses show a less consistent hip-fracture benefit even while vertebral protection stays clear. Bisphosphonates have the most robust hip-fracture evidence, which is one reason they remain first-line when hip risk is the main concern [5].
| Feature | HRT (estrogen-based) | Bisphosphonates |
|---|---|---|
| Main action | Slows bone breakdown by replacing estrogen [3] | Slows bone breakdown by directly suppressing osteoclasts [5] |
| Typical role | Option for women in the menopause window who also want symptom relief; FDA-approved to prevent postmenopausal osteoporosis [1] | Usual first-line treatment for established osteoporosis [5] |
| Fracture protection | Reduced hip and vertebral fractures by about a third in the WHI trial; nonvertebral benefit; hip benefit less consistent in some later analyses [6][3] | Strong reduction across vertebral, nonvertebral, and hip fractures [5] |
| Added benefits | Relieves hot flashes, night sweats, and vaginal dryness; genitourinary and possible early-window cardiovascular benefit [1] | None beyond bone |
| Duration of use | No fixed time limit; protects only while taken [3] | Often 3 to 5 years, then a possible drug holiday; effect lingers in bone [5] |
| Main risks | Blood clots (higher with oral than transdermal); small breast-cancer increase with combined therapy [1] | Stomach upset or reflux (oral); rare osteonecrosis of the jaw and atypical femoral fracture [5] |
| Best-fit patient | Younger postmenopausal woman within 10 years of menopause, especially with symptoms [1] | Older woman, established osteoporosis, or when HRT is not suitable [5] |
Best HRT for osteoporosis: types, forms, and low-dose options
There is no single best hrt for osteoporosis; the right choice depends on your anatomy and your risk profile. The core split is estrogen-only versus combined therapy. Women without a uterus can take estrogen alone. Women who still have a uterus need a progestogen added to protect the lining of the womb (the endometrium) from estrogen [3]. Both regimens protect bone; the progestogen is there for uterine safety, not for the skeleton.
For hrt and bone density, the delivery form also matters. Systemic estrogen comes as a pill, patch, gel, or spray [7], and all of these deliver enough estrogen to protect bone [3]. One important exception: vaginal estrogen, used for local dryness and genitourinary symptoms, keeps blood estrogen levels very low and therefore does not protect the skeleton, so it is not a bone treatment [3]. For many women, transdermal forms (patch, gel, or spray) are preferred because they carry a lower blood-clot risk than tablets, since they bypass the first pass through the liver [1].
Dose is where a common myth needs correcting. When people ask about low-dose hrt for osteoporosis, the reassuring news is that even low-dose HRT protects bone. There is a dose-response, so higher doses generally protect more, but the lowest effective dose still slows bone loss, and as long as you are taking HRT you are helping your bones [3]. That means you and your clinician can often use the smallest dose that controls your symptoms and still get a real benefit for hrt bone density. For a full breakdown of typical starting amounts, see our HRT dosage chart, and for the full menu of regimens, our guide to the types of HRT.
Transdermal versus oral for bone and clot safety: Patches, gels, and sprays deliver estrogen through the skin and avoid the liver first-pass effect, so they raise blood-clot risk far less than tablets while still protecting bone just as well [1]. If clot risk is a concern, transdermal HRT is often the preferred route, and it is worth asking your clinician about specifically.
Who HRT for osteoporosis suits, and who should avoid it
The best candidates for hrt for osteoporosis are perimenopausal and postmenopausal women, especially those under 60 or within 10 years of their last period, women with early or premature menopause, and women who also want relief from menopausal symptoms and have a meaningful fracture risk [1][3]. For these women, using HRT for both symptoms and bone can be an efficient single decision.
Osteoporosis hrt is not right for everyone, though, and some conditions call for caution or make it unsuitable. Your clinician will review your history and generally avoids or carefully weighs HRT if you have a history of breast, ovarian, or uterine cancer; a personal history of blood clots or a high clot risk; active liver disease; a recent heart attack or stroke; unexplained vaginal bleeding; or if you could be pregnant [3][1]. None of this is a self-diagnosis exercise: the point is that a qualified clinician assesses these factors against your bone risk before recommending HRT.
If you and your clinician decide HRT is worth pursuing, our guides on how to get HRT online and how to find an HRT doctor walk through the next steps. Some women also ask about peptides for menopause as an adjacent topic, though these are separate from hormone therapy for bone.
Benefits and risks of HRT for bone: the absolute-risk picture
Good decisions about hormones come from absolute numbers, not headlines. On the benefit side, HRT preserves bone density, lowers fracture risk (in the WHI trial, about a third fewer hip and vertebral fractures) [6], and adds the symptom and genitourinary benefits that bisphosphonates do not provide [1]. On the risk side, the two most-discussed concerns are blood clots and breast cancer, and both are smaller and more specific than reputation suggests.
| Outcome | What HRT does | The absolute picture |
|---|---|---|
| Vertebral and hip fractures | Reduced | About a third fewer hip and vertebral fractures in the WHI trial [6] |
| Blood clots (VTE) | Small increase, oral more than transdermal | Oral estrogen modestly raises an already-low baseline risk; transdermal estrogen at standard doses adds little measurable risk [1] |
| Breast cancer | Small increase, combined therapy only | On the order of fewer than about 1 extra case per 1,000 women per year of combined therapy; estrogen-only therapy is not linked to a rise [1] |
Two distinctions do a lot of work here. First, clot risk depends on the route: tablets carry more risk than skin-based estrogen, so transdermal HRT is often chosen when clots are a concern [1]. Second, breast-cancer risk is tied to combined estrogen-plus-progestogen therapy, is small in absolute terms, and does not apply in the same way to estrogen-only use [1]. For the full treatment of that topic, see our guide to HRT and breast cancer risk.
Regulators have also been re-evaluating older warnings on menopausal hormone therapy, including a move in late 2025 to remove the long-standing boxed warning from these product labels. Because that change is recent and its exact scope matters, confirm the current FDA labeling with your clinician rather than relying on older package inserts. For the broader trade-offs, our overview of hormone replacement therapy and HRT for menopause put the bone benefits in context, and if you are weighing continued use later in life, see taking HRT after 65.
How long HRT takes to work for bone and how long to stay on it
Bone changes slowly, so patience is part of the plan. On a DEXA scan, small gains in bone density usually show up over the first one to three years, and fracture-risk reduction accrues with continued use [3][4]. You will not feel any of this, because bone protection is silent, which is why follow-up scans rather than symptoms guide the timeline. For a fuller walkthrough of what to expect and when, see how long HRT takes to work.
The most important long-term point is that HRT protects bone only while you take it. After stopping, bone loss can resume, and the protection you built up gradually fades, which is why some women transition to a bone-specific drug (such as a bisphosphonate) when they come off HRT, especially if their fracture risk is high [3][5]. That handoff is a planned decision, not an emergency; our guide to stopping HRT covers how clinicians manage the transition so bone stays protected.
Frequently Asked Questions
References
- The Menopause Society (NAMS). The 2022 Hormone Therapy Position Statement. Menopause, 2022. https://menopause.org/professional-resources/position-statements
- Cleveland Clinic Health Essentials. What To Know About Menopause and Bone Loss. Accessed 2026. https://health.clevelandclinic.org/osteoporosis-and-menopause
- Royal Osteoporosis Society. Hormone replacement therapy (HRT) and osteoporosis. Accessed 2026. https://theros.org.uk/information-and-support/osteoporosis/treatment/hormone-replacement-therapy/
- American Academy of Orthopaedic Surgeons. New study finds early hormone replacement therapy reduces risk of osteoporosis and fractures for older women. AAOS 2026 Annual Meeting press release. https://aaos-annualmeeting-presskit.org/2026/research-news/new-study-finds-early-hormone-replacement-therapy-reduces-risk-of-osteoporosis-and-fractures-for-older-women/
- Mayo Clinic. Osteoporosis treatment: Medications can help. Accessed 2026. https://www.mayoclinic.org/diseases-conditions/osteoporosis/in-depth/osteoporosis-treatment/art-20046869
- Writing Group for the Women's Health Initiative Investigators. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women (WHI). JAMA. 2002;288(3):321-333. https://pubmed.ncbi.nlm.nih.gov/12117397/
- MedlinePlus. Hormone Replacement Therapy. U.S. National Library of Medicine. Accessed 2026. https://medlineplus.gov/hormonereplacementtherapy.html
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.