
What should my estradiol level be on HRT? For most menopausal women on estrogen therapy there is no single perfect number, but a commonly cited target is roughly 50 to 100 pg/mL (about 180 to 370 pmol/L), and clinics aiming for fuller symptom and bone protection sometimes target up to 100 to 150 pg/mL. If you are asking what your estrogen level should be on HRT, estradiol (E2) is the estrogen that is actually measured, so this is the number in question. The most important point up front is that guidelines say to dose by how you feel, not by chasing a lab value: your symptoms and side effects lead, and the number is only a supporting tool [1][2]. This guide is about menopausal hormone therapy for women, not transgender care or men's therapy, which use different targets.
🔑 Key Takeaways
- The common target is about 50 to 100 pg/mL. For menopausal women on estrogen therapy this range (roughly 180 to 370 pmol/L) is the window most sources converge on, with some optimization clinics aiming up to 100 to 150 pg/mL [1].
- There is no single correct number. Response is individual, and major guideline bodies do not recommend routine blood testing to steer standard menopausal HRT [1][2].
- Symptoms outrank the reading. ACOG, the Menopause Society, and ESHRE judge HRT by symptom relief and side effects, not by hitting a target estradiol value [1][2][3].
- Delivery method changes the number. Oral estradiol raises estrone and under-represents tissue exposure, transdermal gives steadier readings, and injections and pellets peak then trough [4][6].
- Units differ by country. The US reports pg/mL; the UK, Europe, Canada, and Australia report pmol/L, and 1 pg/mL is about 3.67 pmol/L [7].
| Quick fact | What it means |
|---|---|
| Untreated postmenopausal estradiol is typically under 10 to 20 pg/mL | HRT aims to lift E2 into a therapeutic window, not to reach a premenopausal peak [5][6] |
| Common on-HRT target is about 50 to 100 pg/mL (180 to 370 pmol/L) | The range most menopause sources agree on for symptom and bone benefit [1] |
| Guidelines advise dosing by symptoms, not by lab number | Routine estradiol monitoring is not recommended for standard HRT [1][2] |
| 1 pg/mL is about 3.67 pmol/L | The conversion you need to compare US and UK or European targets [7] |
What should my estradiol level be on HRT? (the short answer)
So, what should estradiol levels be on HRT for a menopausal woman? The honest answer is that there is no universal correct figure, but the practical target that most menopause sources land on is about 50 to 100 pg/mL, which is roughly 180 to 370 pmol/L [1]. Some clinics that focus on hormone optimization aim a bit higher, toward 100 to 150 pg/mL, arguing it gives fuller symptom control and stronger bone protection, though that upper band sits above the conservative guideline window and is not something every clinician targets [1].
The headline number, with the caveat that comes with it: roughly 50 to 100 pg/mL (about 180 to 370 pmol/L) is the commonly cited target on HRT, and up to 100 to 150 pg/mL is an optimization target used by some clinics. It is individualized, and guidelines say to treat the person and the symptoms, not the lab result [1][2].
Two things trip people up. First, estrogen is a family of hormones, and the one measured on a blood test is estradiol (E2), the main and most active estrogen in women of reproductive age [6]. When a clinician talks about your estradiol level, that is your estrogen level for this purpose. Second, the units are different depending on where you live: the United States reports pg/mL, while the UK, most of Europe, Canada, and Australia report pmol/L [7]. That is why a UK reader who sees a target of 180 to 370 pmol/L and a US reader who sees 50 to 100 pg/mL are looking at the same range. The conversion table further down turns one into the other.
Optimal estradiol levels postmenopausal on HRT
To understand what an optimal estradiol level postmenopausal on HRT looks like, it helps to see the starting point. After menopause the ovaries largely stop making estradiol, and an untreated postmenopausal level is typically low, often under 10 to 20 pg/mL (under about 37 to 73 pmol/L) [5][6]. That is the level associated with hot flashes, night sweats, disrupted sleep, and ongoing bone loss. The aim of HRT is not to recreate a young woman's peak but to lift estradiol into a steady therapeutic window that eases symptoms and protects bone [1].
Where inside that window matters. Menopause clinicians and the wider literature commonly describe estradiol around 60 pg/mL (about 220 pmol/L) as a level linked with hot-flash relief in roughly half of women and with slowing of the bone loss that speeds up after menopause, while levels closer to 100 pg/mL (about 367 pmol/L) are associated with fuller symptom relief [1]. These are associations reported across menopause practice rather than a fixed prescription, and where any individual woman feels her best varies. The framing that guidelines are comfortable with is directional: too low and symptoms and bone loss persist, comfortably inside the window and most women do well, without a magic setpoint everyone must hit.
| E2 level | What research and menopause practice associate with it |
|---|---|
| Under 20 pg/mL (under ~73 pmol/L) | Typical of untreated menopause; hot flashes, sleep disruption, and ongoing bone loss are common |
| About 60 pg/mL (~220 pmol/L) | Commonly cited with hot-flash relief in roughly half of women and with slowing of bone loss |
| About 100 pg/mL (~367 pmol/L) | Associated with fuller hot-flash relief |
| 100 to 150 pg/mL (~367 to 551 pmol/L) | Target used by some optimization clinics; sits above the conservative guideline window |
*These associations come from clinical literature and menopause practice. They are individualized and are not a prescription; specific thresholds vary between studies, so confirm what applies to you with your clinician.* Bone protection is one of the clearest reasons the window matters, and our guide to HRT and osteoporosis covers how estrogen preserves bone density in more detail.
Estradiol levels on HRT by delivery method
Talking about estradiol levels on HRT without naming the delivery method leaves out half the story, because how you take estrogen changes both the reading and how useful that reading is. The same target range applies in principle, but HRT estrogen levels behave differently by route [4][6].
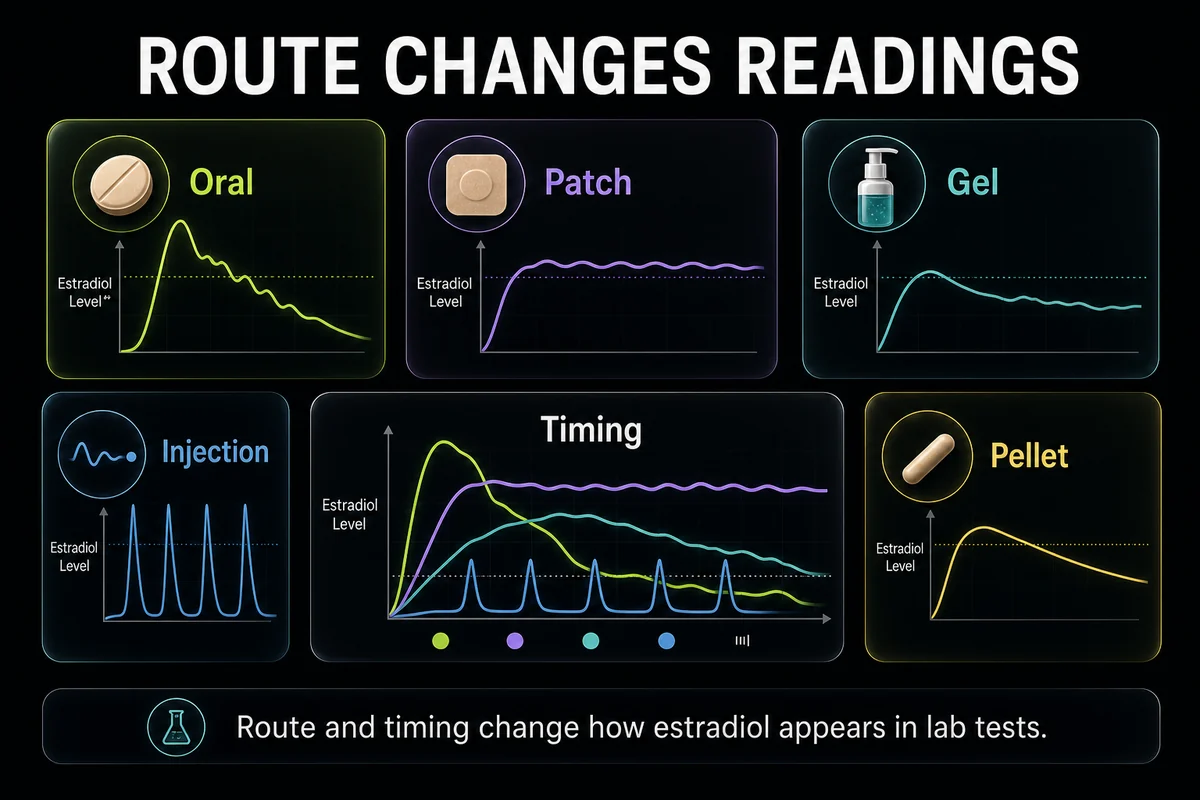
Oral estradiol passes through the liver first (the first-pass effect). That metabolism converts a large share of it into estrone (E1), another estrogen, so a blood estradiol reading on oral therapy under-represents the total estrogen effect your tissues are getting [6]. For this reason a single E2 number is less informative on tablets, and clinicians lean even more heavily on symptoms.
Transdermal estradiol (patch, gel, or spray) is absorbed through the skin and skips the first-pass liver step, so serum estradiol tends to track more steadily and is more representative [4]. This is also where testing earns its keep: some women are so-called poor absorbers who need a higher dose to reach the target window through the skin, and a mid-interval blood test can confirm whether absorption is adequate. Our guide to estradiol patches goes deeper on absorption, and the wider menu of routes is covered in types of HRT.
Injectable estradiol and pellets produce peaks and troughs rather than a flat line. An injection can push levels high soon after dosing and let them fall before the next dose, and a pellet tends to run higher in the weeks after insertion then decline over months, so any reading has to be interpreted against the timing rather than compared to a fixed target [4].
| Delivery method | Common target serum E2 | Same in pmol/L | Testing note |
|---|---|---|---|
| Oral estradiol | About 50 to 100 pg/mL (aim by symptoms) | About 180 to 370 | Blood E2 under-represents effect because oral dosing raises estrone; testing is least informative |
| Transdermal patch | About 50 to 100 pg/mL | About 180 to 370 | Steadier levels; test mid-patch-interval to check absorption |
| Transdermal gel or spray | About 50 to 100 pg/mL | About 180 to 370 | Steady if applied consistently; test at a consistent time after application |
| Injectable estradiol | Varies with timing (peak then trough) | Varies | Interpret against injection timing, not a fixed target |
| Pellet | Varies (higher early, falls over months) | Varies | Levels peak after insertion then decline; read by timing since insertion |
*The 50 to 100 pg/mL window reflects the guideline consensus rather than a method-specific promise. Injectable and pellet levels swing too much for a single target figure, so confirm the right interpretation with your clinician.* How a given dose maps onto these numbers is covered in our HRT dosage chart.
pg/mL vs pmol/L: estradiol unit conversion
If you are comparing a US target with a UK or European one, you need the estradiol unit conversion, and this is the piece most pages leave out. Both units measure the same thing: pg/mL (picograms per milliliter) is a mass concentration, and pmol/L (picomoles per liter) is a molar concentration. Because estradiol has a molecular weight of about 272, one converts to the other with a fixed factor.
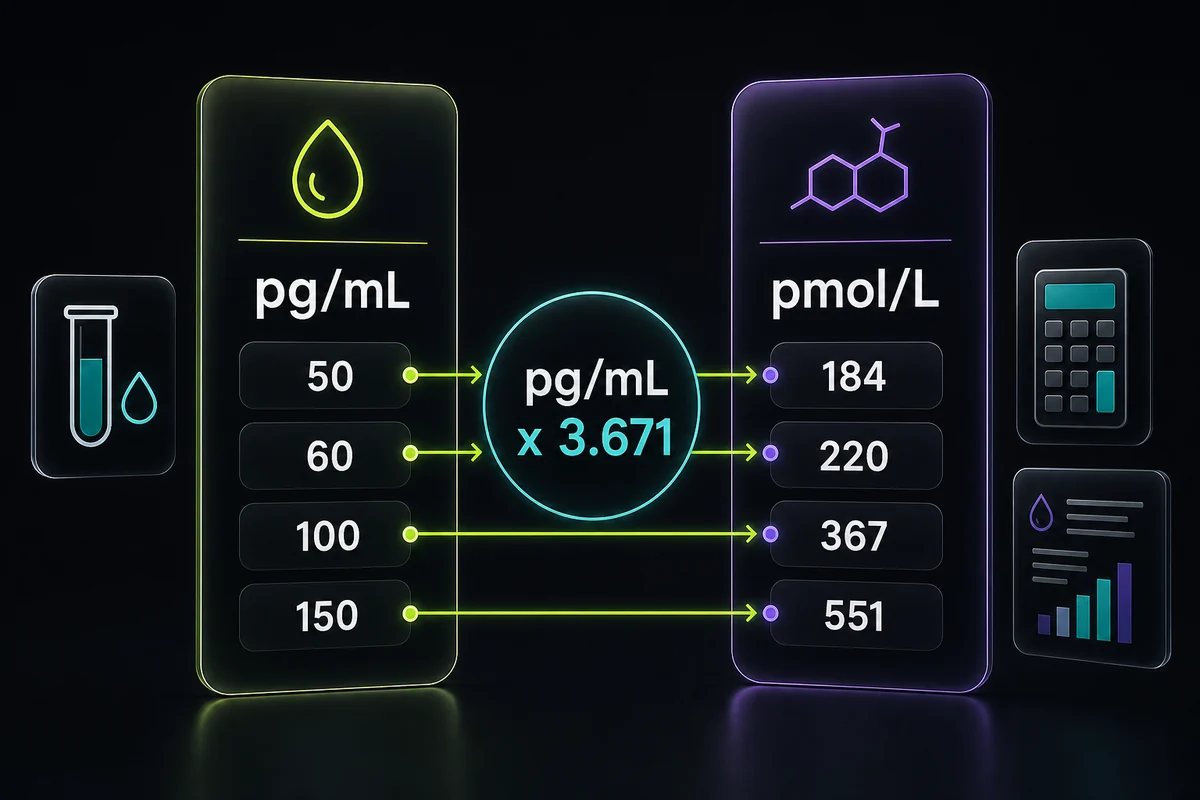
The conversion factor: pg/mL x 3.671 = pmol/L, and pmol/L divided by 3.671 = pg/mL. So a US target of 50 to 100 pg/mL is about 180 to 370 pmol/L.
| pg/mL | pmol/L | Context |
|---|---|---|
| 10 | 37 | Typical untreated postmenopausal level |
| 30 | 110 | Below the usual on-HRT target |
| 50 | 184 | Low end of the common on-HRT target |
| 60 | 220 | Often-cited bone and hot-flash threshold |
| 100 | 367 | Associated with fuller symptom relief |
| 150 | 551 | Upper optimization-clinic target |
| 200 | 734 | Generally above the menopausal target range |
This matters in practice because UK guidance and UK and European labs report in pmol/L [7]. A woman reading a British forum that talks about aiming for 250 to 400 pmol/L and an American reading about 70 to 110 pg/mL are discussing broadly the same territory once you convert. Keep the factor of 3.671 handy and the two number systems stop being confusing.
Why estradiol levels matter less than symptoms on HRT
Here is the part that reconciles the whole topic. When people search for the ideal hormone levels on HRT or the target hormone levels for HRT, they are often surprised to learn that the major guideline bodies do not recommend routinely measuring estradiol to run standard menopausal HRT at all. ACOG, the Menopause Society, ESHRE, and NICE all take the position that treatment is judged by symptom relief and the absence of troublesome side effects, not by hitting a blood level [1][2][3][7]. NICE, for example, advises against using blood hormone tests to guide menopause treatment in most women [7]. The dose that controls your hot flashes, protects your sleep, and does not cause side effects is, for guideline purposes, the right dose, whatever the number reads.
There is a reasonable counter-view, and it is worth stating fairly. Some clinicians do check estradiol in specific situations: to confirm absorption in a transdermal user whose symptoms are not improving, when bone loss continues despite treatment, or after a dose change [3][7]. Hormone-optimization clinics go further and titrate to a target range. Neither approach is fringe, but it is a narrower, selective use of testing rather than the routine monitoring many people assume happens.
The balanced takeaway: the estradiol number is a tool, not the goal. For most women on HRT, symptoms and clinician judgment lead, and a blood test is used selectively, for example to check absorption or investigate persistent symptoms. Chasing a specific figure for its own sake is not what guidelines advise [1][2][3].
When and how to test your estradiol on HRT
If testing is on the table, it helps to know who tends to benefit and how to do it well. Blood estradiol is most useful for women with symptoms that will not settle on a reasonable dose, transdermal users checking whether they are absorbing enough, women with ongoing bone-density concern, and anyone reviewing the effect of a recent dose change [3][7]. For many women who feel well on HRT, no test is needed at all.
Timing and method matter as much as the decision to test. Patch users should test mid-interval rather than right after a change, gel or spray users should test at a consistent time relative to when they apply, and oral testing is the least informative because of the estrone effect [4][6]. Ask specifically for a serum estradiol (E2, sometimes labeled 17-beta-estradiol) rather than a total estrogen panel, and be aware that an ultrasensitive assay (LC-MS/MS) is more accurate at the low levels seen after menopause [5]. If testing is indicated at all, many clinicians wait until you have been on a stable dose for about three months so levels have settled, which our guide to how long HRT takes to work explains further.
Reading the result is where a clinician earns their keep. A level that is too low usually shows up as persistent symptoms and, over time, continued bone loss, and it may prompt a dose increase or a switch of route [1]. A level that is high on its own is not an emergency, but it warrants a symptom and dose review to check for side effects, and it is a reminder of a separate safety rule: women who still have a uterus need adequate progestogen alongside estrogen to protect the uterine lining, regardless of the estradiol number [2]. Unexpected bleeding always deserves attention, which our guide to bleeding on HRT covers, and the fuller side-effect picture is in HRT side effects. If you want a provider who includes lab work, our roundup of online HRT providers that include lab testing and our guide to finding an HRT doctor near you are good next steps.
Estradiol targets in context: age, weight, and progesterone
A target range is a starting point, not a fixed rule, because several personal factors shift where you land and what it means. Body fat is one: fat tissue converts other hormones into estrogen (aromatization), so women with a higher BMI often carry a somewhat higher baseline estradiol even before treatment, and their dosing may differ from a leaner woman aiming for the same symptom relief [6]. Age and time since menopause also matter, since the point of therapy and the balance of benefits and risks shift the further you are from your last period, a theme covered across our HRT for menopause and HRT for perimenopause guides.
Progesterone deserves its own line because it is a safety point, not a level target. If you have a uterus, estrogen taken on its own can overstimulate the uterine lining, so a progestogen is added to protect it, and that protection is judged by the regimen and by the absence of abnormal bleeding rather than by chasing a progesterone number [2]. In other words, the estradiol target answers "is the estrogen dose doing its job," while the progestogen answers a separate question about keeping the lining safe. Both belong in the conversation with your clinician, and neither is something to self-manage from a lab printout, which is the throughline of the whole topic and the pillar guide to HRT for women.
Frequently Asked Questions
References
- The Menopause Society (NAMS). The 2022 Hormone Therapy Position Statement. Menopause, 2022. https://menopause.org/professional-resources/position-statements
- American College of Obstetricians and Gynecologists (ACOG). Hormone Therapy for Menopause Symptoms. Accessed 2026. https://www.acog.org/womens-health/faqs/hormone-therapy-for-menopause-symptoms
- European Society of Human Reproduction and Embryology (ESHRE). Guideline on the Management of Premature Ovarian Insufficiency. Accessed 2026. https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Premature-Ovarian-Insufficiency
- Mayo Clinic. Estradiol (Transdermal Route). Accessed 2026. https://www.mayoclinic.org/drugs-supplements/estradiol-transdermal-route/description/drg-20075306
- MedlinePlus. Estrogen Levels Test. U.S. National Library of Medicine. Accessed 2026. https://medlineplus.gov/lab-tests/estrogen-levels-test/
- Cleveland Clinic. Estrogen. Accessed 2026. https://my.clevelandclinic.org/health/body/22353-estrogen
- National Institute for Health and Care Excellence (NICE). Menopause: diagnosis and management (NG23). Accessed 2026. https://www.nice.org.uk/guidance/ng23
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.