
There is no single best age for TRT, and no medical guideline sets a minimum age, because testosterone replacement therapy is prescribed for a confirmed diagnosis, not for a birthday. The bar is the same at 25 as it is at 65: symptoms of low testosterone plus a total testosterone below 300 ng/dL (about 10.4 nmol/L) on two separate morning blood draws, with reversible causes ruled out, as described by the AUA and the Endocrine Society 12. So the honest answer to "best age for TRT" is that age informs the decision but never settles it. A few YMYL guardrails frame everything below: testosterone is a prescription, Schedule III controlled therapy; the FDA has approved it only for hypogonadism caused by medical conditions, not for low testosterone due to normal aging 56; and every number here is educational, with your candidacy, target, and dose set by your prescriber from your own labs and symptoms. If TRT is new to you, start with our pillar guide to testosterone replacement therapy.
Key Takeaways
- There is no "best age" and no minimum age for TRT. No guideline defines one, because candidacy is a diagnosis, not a birthday 12.
- Diagnosis decides it, not age. The qualifier is symptoms plus a total testosterone below 300 ng/dL (about 10.4 nmol/L) on two separate morning draws, with reversible causes ruled out 28.
- The FDA has not approved testosterone for age-related low T. It is approved for hypogonadism from certain medical conditions, not for the normal dip that comes with aging 56.
- Younger men should settle fertility first. Exogenous testosterone suppresses sperm production, so the fertility question comes before starting, not after 12.
- Testosterone falls only about 1 to 1.6 percent per year after 30 to 40. A low level in a young man usually has a specific, sometimes reversible cause rather than "just aging" 310.
- TRT does not make you biologically age faster. It can change skin, hair, and fluid balance, but there is no evidence it accelerates aging, and it is not a proven anti-aging therapy 1011.
- TRT is typically a lifelong commitment. Because it suppresses your own production, the decision at any age is a long-term one 1.
| Metric | Value |
|---|---|
| Guideline-defined minimum age | None; candidacy is a diagnosis, not a birthday 12 |
| Diagnostic cutoff | Total testosterone below 300 ng/dL (about 10.4 nmol/L) on two morning draws, plus symptoms 2 |
| FDA-approved use | Hypogonadism from certain medical conditions, not low testosterone due to aging 56 |
| Natural decline after 30 to 40 | About 1 percent per year (about 1.6 percent per year total, 2 to 3 percent bioavailable) 310 |
| Prevalence of low levels | Roughly 20 percent of men in their 60s, 30 percent in their 70s, 50 percent in their 80s 4 |
| Under-18 use | Not indicated; safety and efficacy not established 7 |
| Does TRT age you | No evidence it accelerates biological aging 1011 |
Is There a Best Age for TRT?
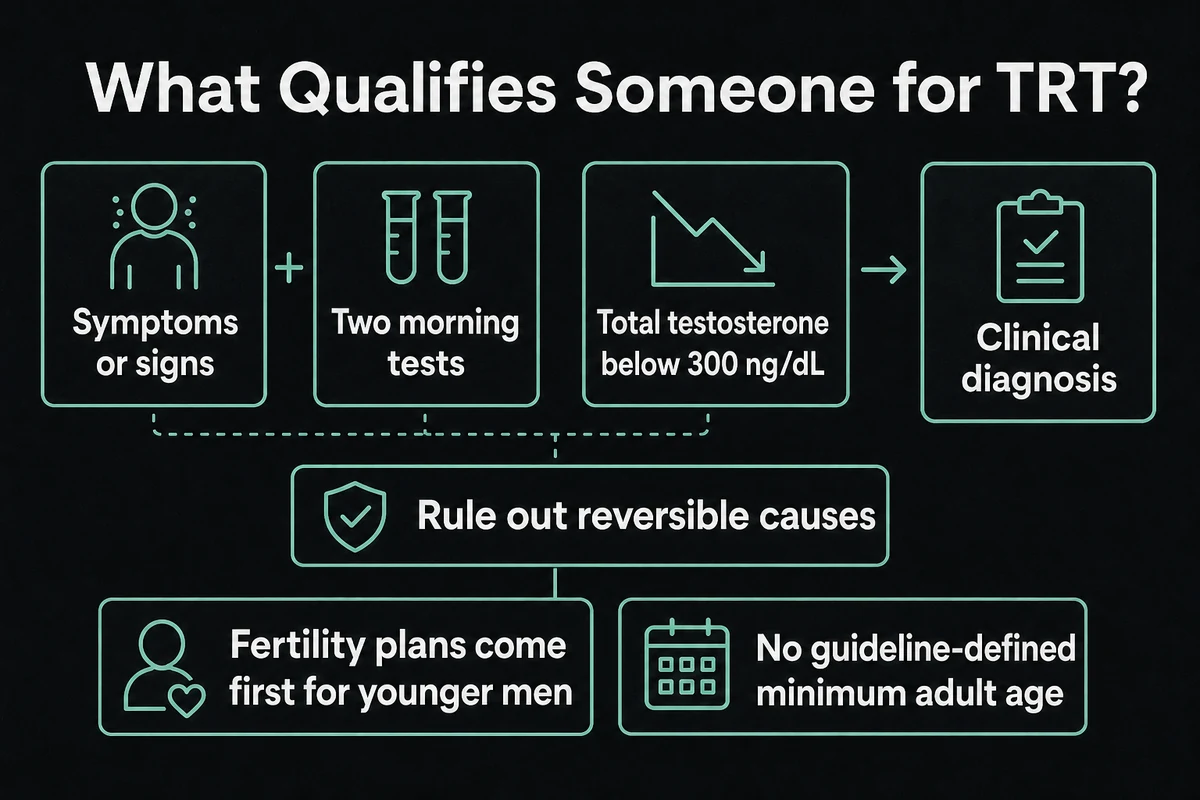
The search behind "best age for trt," "best age to start trt," "at what age is trt recommended," "what age is trt recommended," and "trt therapy age" is usually looking for a number, and the useful answer is that no number exists. No major guideline names a "best" age or a minimum age to start testosterone therapy, because the therapy is tied to a diagnosis, not to a stage of life. The AUA and the Endocrine Society define testosterone deficiency the same way regardless of age: consistent symptoms of low testosterone together with a total testosterone below 300 ng/dL (about 10.4 nmol/L), confirmed on two separate early-morning blood draws, with reversible causes excluded first 12. Age changes how hard your clinician looks for a cause, but it is never the qualifier by itself.
Layered on top of the guideline definition is a fact that no TRT clinic on this topic tends to state plainly: the FDA has approved testosterone products only for men with hypogonadism due to certain medical conditions, and specifically not for low testosterone caused by aging 56. In its class-wide labeling changes, the FDA kept the indication to diagnosed hypogonadism and added a blood-pressure warning 5. That distinction is the whole game. A gradual, expected decline into your 40s or 50s is not, on its own, a medical indication, while a genuine deficiency at 28 can be. To understand what the numbers mean once you are looking at your own bloodwork, see our guide to testosterone levels on TRT; for the full picture of the therapy itself, the testosterone replacement therapy pillar walks through diagnosis, formulations, and monitoring. A quick unit note used throughout: US labs report ng/dL, the rest of the world uses nmol/L, and you convert by multiplying ng/dL by 0.0347.
What Age to Start TRT: Diagnosis, Not a Number
For "what age to start trt," "age to start trt," "what age should you start trt," "age for trt," and "trt age," the decision walks through the same checklist at any age. First, a confirmed low morning testosterone (below 300 ng/dL, or about 10.4 nmol/L) on two separate draws. Second, real symptoms that fit, such as low libido, fatigue, erectile changes, low mood, or loss of morning erections. Third, reversible causes ruled out, because weight, sleep, alcohol, opioids, thyroid, and pituitary issues can all lower testosterone 18. Fourth, the tradeoffs understood, chiefly the fertility question and the reality that TRT is usually lifelong. Only when those line up does starting make sense.
Age informs the workup rather than the verdict. In a younger man, a low reading should prompt a harder search for a specific cause before anyone reaches for a prescription, while in an older man the same low reading is more expected but still has to pair with symptoms to justify treatment. If your numbers are borderline or your symptoms are vague, non-testosterone routes may fit better, and our overview of TRT alternatives covers those options.
How Testosterone Changes With Age (TRT Levels by Age)
To read "trt levels by age" and "trt age" correctly, start with the normal trajectory. Testosterone peaks in the late teens and early 20s, then declines slowly. Mayo Clinic and Harvard Health both put the fall at roughly 1 percent per year after age 30 to 40 1011. Longitudinal data sharpen that: in the Massachusetts Male Aging Study, total testosterone dropped about 1.6 percent per year and bioavailable (free plus loosely bound) testosterone about 2 to 3 percent per year within individual men 3. The Baltimore Longitudinal Study of Aging found hypogonadal levels in roughly 20 percent of men in their 60s, 30 percent in their 70s, and 50 percent in their 80s 4. For a reference band, the harmonized normal range for healthy nonobese men aged 19 to 39 is 264 to 916 ng/dL (about 9.2 to 31.8 nmol/L), with a median of 531 ng/dL (about 18.4 nmol/L) 13.
The point that gets lost in marketing is this: a gradual, normal decline is not the same thing as hypogonadism. A mildly low-normal number in a man with no symptoms is not a TRT indication, and MedlinePlus notes that testosterone naturally declines with age and that a single reading has to be interpreted in context, not treated in isolation 9. The table below stratifies the trend and the key consideration by decade. For how those numbers translate into targets on therapy, see testosterone levels on TRT.
| Age band | Typical testosterone trend | What low T usually means at this age | Key consideration |
|---|---|---|---|
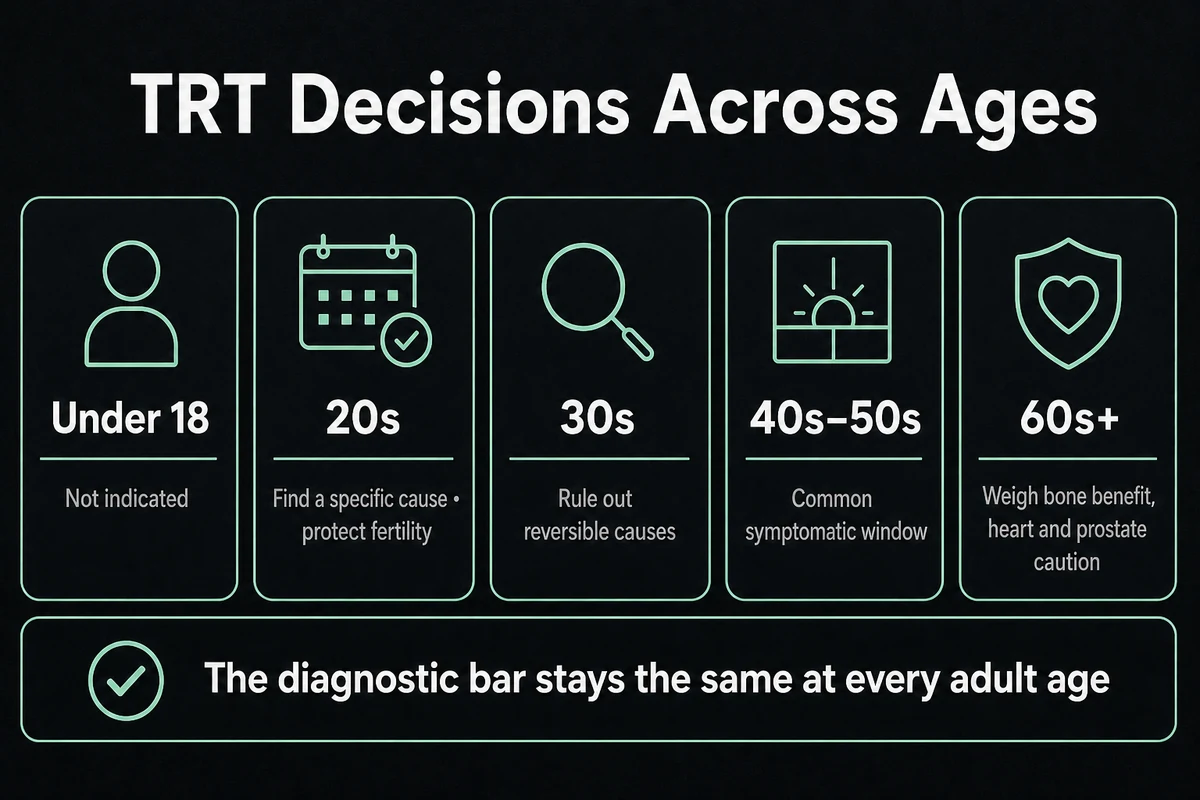
| Under 18 | Rising through puberty | A pubertal or medical issue, managed by pediatric endocrinology | Testosterone products are not indicated under 18 7 |
| 20s | Near lifetime peak | Uncommon; almost always a specific cause | Rule out and treat causes first; protect fertility 8 |
| 30s | Gradual decline begins (about 1 to 1.6 percent per year) | Often a reversible cause; confirmed hypogonadism is valid | Exclude reversible causes; fertility; lifelong commitment 38 |
| 40s to 50s | Continued decline; symptoms become meaningful | The most common symptomatic starting window | Same diagnostic bar; monitoring begins 3 |
| 60s+ | Highest prevalence of low levels | Age-related plus medical causes | Bone benefit weighed against cardiovascular and prostate caution 412 |
TRT in Your 20s
For "trt in 20s" and "trt in your 20s," the headline is that genuinely low testosterone at this age is uncommon, and when it shows up it almost always has a specific, identifiable cause. Cleveland Clinic groups these into primary hypogonadism (the testicles themselves, from genetic conditions such as Klinefelter syndrome, undescended testes, injury, infection, or chemotherapy) and secondary hypogonadism (the pituitary or hypothalamus, plus obesity, opioids, and prior anabolic-steroid use) 8. The guideline-mandated first step is to find and treat what is reversible, not to reach straight for lifelong replacement 1.
Two considerations weigh most heavily in your 20s. The first is fertility: exogenous testosterone suppresses the body's own signaling and can shut down sperm production, so if you may want children, that conversation comes before you start, not after. Our guide to TRT and fertility covers why, and enclomiphene is one fertility-preserving option that raises your own testosterone instead of replacing it. The second is the under-18 edge: testosterone products are not indicated in males under 18 because safety and efficacy have not been established, and adolescents with hormonal concerns are managed by pediatric endocrinology, not by TRT clinics 7.
TRT in Your 30s
"TRT in 30s," "trt in your 30s," "trt for 30 year old," "trt age 30," and "is 30 too young for trt" together make this the highest-volume decade in the cluster, so it deserves a direct answer. Is 30 too young for TRT? No, age is not the disqualifier, and a confirmed diagnosis at 30 is a legitimate, evidence-based indication. But at 30 you first do the work that a good clinician insists on: exclude the reversible causes that are common at this age, including excess weight, obstructive sleep apnea, heavy alcohol use, opioids, prior anabolic-steroid use, and thyroid or pituitary problems 128. Many men in their 30s who feel "low" are carrying one of these, and fixing it can lift testosterone without any prescription at all.
The distinction that matters is between confirmed hypogonadism and low-normal-with-vague-symptoms. A total testosterone below 300 ng/dL (about 10.4 nmol/L) on two morning draws, with fitting symptoms and reversible causes ruled out, is a real indication at 30 2. A borderline number attached to fatigue that could stem from sleep, stress, or training load is not. Because a 30-year-old is likely looking at decades of therapy, the two tradeoffs loom large: fertility (see TRT and fertility, and hCG as a way to maintain the testes' own function) and the lifelong nature of the commitment, which our guide to stopping TRT explains in practical terms.
TRT in Your 40s and 50s
By the 40s and 50s, symptomatic decline becomes clinically meaningful for more men, which is why this is the most common starting window and a big share of "age for trt" searches. The diagnostic bar does not loosen: it is still symptoms plus a confirmed low morning level with reversible causes excluded 12. What changes is that a genuine deficiency is simply more likely, and the potential benefits (improvements in energy, libido, mood, body composition, and bone density in men who are truly deficient) are more often on the table. Our guide to TRT benefits covers what the evidence does and does not support.
This is also where monitoring starts to matter more, because testosterone raises red blood cell count and can affect the prostate and blood pressure. Standard follow-up tracks hematocrit, PSA, and blood pressure on a schedule, and the FDA's 2025 labeling update added a blood-pressure warning to the class 5. Our page on TRT side effects walks through what is monitored and why, so the risks stay managed rather than ignored.
TRT After 60
For "at what age is trt recommended" from the older-adult angle, prevalence of low testosterone is highest here, with hypogonadal levels in roughly 20 percent of men in their 60s and rising further with age 4. The bone-density benefit of correcting a true deficiency is most clinically meaningful in this group. But the framing has to be absolute risk, not hype. In the TRAVERSE trial, testosterone therapy in hypogonadal men aged 45 to 80 with cardiovascular risk was noninferior to placebo for major adverse cardiac events, while showing higher rates of atrial fibrillation, pulmonary embolism, and acute kidney injury 12. Prostate and PSA monitoring also matter more with age 7.
The most important point for older men is one Mayo Clinic states plainly: testosterone is not an anti-aging therapy, and the benefits of treating the normal age-related decline (as opposed to a diagnosed deficiency) are not clear 10. So after 60 the decision is still diagnosis-led, with the added weight of cardiovascular and prostate monitoring. For those specifics, see TRT and heart health and TRT and prostate cancer.
Does TRT Age You? Skin, Hair, and Looking Older or Younger
This sub-cluster ("does trt age you," "does trt make you look older," "does trt make you look younger," "does trt make you age faster," and "trt age") is answered almost nowhere with real dermatology, so here is the factual version. Testosterone does change skin and appearance in ways that are cosmetic, not evidence of changed biological aging. It thickens the dermis and raises collagen and sebum, which can firm skin but also cause acne and oiliness. Fluid and sodium retention can puff the face. A higher hematocrit and vasodilation can flush the skin. And in men who are genetically susceptible, testosterone can accelerate male-pattern hair loss, which reads to many people as "looking older."
What none of that supports is the idea that TRT ages you faster at the biological level, or the opposite marketing claim that it is a "look younger" or anti-aging treatment. There is no evidence TRT accelerates aging, and Mayo Clinic and Harvard Health are clear that testosterone is not a fountain of youth and its benefits for age-related decline are not established 1011. The reports on both sides ("it aged my face," "it made me look younger") are real but individual and cosmetic. The hair question specifically is covered in TRT and hair loss, and the broader skin and fluid effects in TRT side effects.
| Claim | What the evidence shows |
|---|---|
| "TRT ages your face" | Fluid retention, acne, and a higher hematocrit can change appearance, but there is no evidence of faster biological aging 1011 |
| "TRT makes you look younger / is anti-aging" | Not a proven anti-aging therapy; benefits for age-related decline are not clear 10 |
| "TRT causes hair loss" | Can accelerate male-pattern hair loss only in genetically susceptible men (see TRT and hair loss) |
| "TRT makes you age faster" | No evidence; the effects on appearance are cosmetic and individual 1011 |
Does TRT Make You Look Older or Younger?
Resolving "does trt make you look older," "does trt make you look younger," and "does trt make you age faster" directly: both experiences are cosmetic and individual, driven by fluid balance, acne, hematocrit, hair pattern, and shifts in fat and muscle, not by any change to how fast your body ages. Someone who retains fluid and flushes may feel they look puffier or ruddier; someone who loses fat and gains a little muscle may feel they look leaner and fresher. Neither is TRT working as a cosmetic or anti-aging product, and it should never be presented or pursued as one.
Reversible Causes to Rule Out Before Starting TRT (Any Age)
The step most competitor pages skip is the one the guidelines put first: rule out and address reversible causes before committing to lifelong therapy, at any age 18. Losing excess weight, treating obstructive sleep apnea, cutting back alcohol, reducing or reviewing opioids, and correcting thyroid or pituitary issues can each raise testosterone without a prescription. In a younger or borderline case, this is not a delay tactic, it is the correct medicine.
For men who want to preserve fertility, there are prescription routes that raise your own testosterone instead of replacing it. Enclomiphene and hCG stimulate the body's own production and keep the testes working, which exogenous testosterone does not, and our comparison of sermorelin, MK-677, and enclomiphene explains where each fits. Our overview of TRT alternatives compares the routes, and enclomiphene and hCG go deeper on each. What does not belong in this conversation is over-the-counter "testosterone boosters," which do not meaningfully move these numbers, as our look at testosterone boosters versus peptides details.
Is TRT a Lifelong Commitment?
For most men, yes. Exogenous testosterone suppresses the body's own production through the same feedback loop that causes fertility suppression, so stopping usually returns you to your baseline low, or lower for a period, while the system recovers 12. That is why the decision to start, at 30 or at 60, is a long-term one and not a trial you casually reverse. Our guide to stopping TRT covers what discontinuation actually looks like and why the choice deserves the same care as starting.
Frequently Asked Questions
There is no best age. No guideline sets a minimum, because TRT is prescribed for a confirmed diagnosis, not a birthday: symptoms plus a total testosterone below 300 ng/dL (about 10.4 nmol/L) on two separate morning draws, with reversible causes ruled out 12. Age informs how hard your clinician looks for a cause, but it never qualifies you on its own.
Yes, if there is a confirmed diagnosis, but low testosterone in your 20s is uncommon and almost always has a specific cause (genetic conditions, injury, pituitary problems, obesity, opioids) that should be identified and treated first 8. Fertility weighs especially heavily this young, so discuss fertility-preserving options like enclomiphene or hCG before exogenous testosterone 1.
No, TRT is not a proven anti-aging or "look younger" therapy, and Mayo Clinic notes its benefits for age-related decline are not clear 10. Some men feel they look leaner or fresher from changes in fat and muscle, but that is an individual cosmetic effect, not TRT working as an anti-aging treatment.
TRT is not recommended at any particular age; it is recommended for a diagnosis. The prevalence of low levels rises with age (roughly 20 percent of men in their 60s, 30 percent in their 70s, 50 percent in their 80s), but the same criteria apply throughout, and the FDA has not approved testosterone for age-related low T 456.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432.
- Feldman HA, et al. Age Trends in the Level of Serum Testosterone and Other Hormones in Middle-Aged Men: Massachusetts Male Aging Study. J Clin Endocrinol Metab. 2002;87(2):589-598.
- Harman SM, et al. Longitudinal Effects of Aging on Serum Total and Free Testosterone Levels in Healthy Men (Baltimore Longitudinal Study of Aging). J Clin Endocrinol Metab. 2001;86(2):724-731.
- U.S. Food and Drug Administration. FDA issues class-wide labeling changes for testosterone products. 2025.
- U.S. Food and Drug Administration. Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging. March 2015 (indexed reprint).
- U.S. Food and Drug Administration. AndroGel 1.62% (testosterone gel) Prescribing Information. 2016.
- Cleveland Clinic. Low Testosterone (Male Hypogonadism). Accessed 2026.
- MedlinePlus. Testosterone Levels Test. U.S. National Library of Medicine. Accessed 2026.
- Mayo Clinic. Testosterone therapy: Potential benefits and risks as you age. Accessed 2026.
- Harvard Health Publishing. Testosterone: What it does and doesn't do. Accessed 2026.
- Lincoff AM, Bhasin S, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023;389(2):107-117.
- Travison TG, et al. Harmonized Reference Ranges for Circulating Testosterone Levels in Men of Four Cohort Studies. J Clin Endocrinol Metab. 2017;102(4):1161-1173.
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.