
Does TRT cause blood clots? For some men, yes, and the honest, guideline-anchored answer is that testosterone can modestly raise clot risk, concentrated in the first few months and driven mainly because it raises your red blood cell count and thickens your blood. That risk is real but usually small in absolute terms, and it is the reason the U.S. Food and Drug Administration added a class-wide blood-clot (venous thromboembolism) warning to every testosterone product in February 2025, at the same time it removed the older boxed cardiovascular warning 1. Held next to that caution is a reassuring headline: the large TRAVERSE trial found no increase in heart attacks, strokes, or cardiovascular deaths on testosterone 2. Both facts are true at once. This page fuses the three cardiovascular jobs most articles split across separate pages, clots, cholesterol, and heart rate and rhythm, so you can see the whole picture with real numbers, guideline thresholds, and resolvable citations. Used with proper lab monitoring, these risks are monitorable and largely manageable, not usually a reason to avoid testosterone replacement therapy.
Key Takeaways
- Clots are a real but small and early risk: the extra clot risk is modest in absolute terms and front-loaded to the first few months after starting, driven by a rising red blood cell count rather than a mysterious direct effect 511.
- TRAVERSE found no rise in major cardiac events: major adverse cardiac events were 7.0% on testosterone versus 7.3% on placebo (non-inferior), but the same trial recorded more atrial fibrillation, pulmonary embolism, and acute kidney injury on testosterone 2.
- The FDA rewrote the label in February 2025: it removed the boxed cardiovascular warning and added a new class-wide venous-thromboembolism (blood clot) warning plus a blood-pressure warning to every testosterone product 1.
- Hematocrit is the main clot lever: testosterone raises red blood cell production, which thickens the blood, so the percentage of your blood that is red cells (hematocrit) is the number your clinician watches most closely 311.
- Cholesterol changes are modest at TRT doses: at physiologic replacement doses, lipids typically shift a little, a small HDL dip alongside neutral-to-lower total and LDL cholesterol, very different from the sharp changes seen with anabolic-steroid abuse 8.
- Monitoring makes it manageable: testosterone and hematocrit are checked at baseline, at 3 to 6 months, at 12 months, and then annually, which is what turns a list of risks into a managed plan 34.
Does TRT cause blood clots?
Yes, testosterone replacement therapy can cause blood clots in some men, and that risk is now written directly into the drug labels. In February 2025 the FDA issued class-wide labeling changes for testosterone products, adding a warning about venous thromboembolism, meaning deep vein thrombosis (DVT) and pulmonary embolism (PE), to every product in the class 1. The patient-facing label language says the same thing in plainer terms: MedlinePlus lists blood clots, along with high red blood cell counts and a raised risk of heart attack or stroke, among the precautions for testosterone 7. This is not a brand-new discovery either, the FDA first flagged a possible clot signal back in 2014 6.
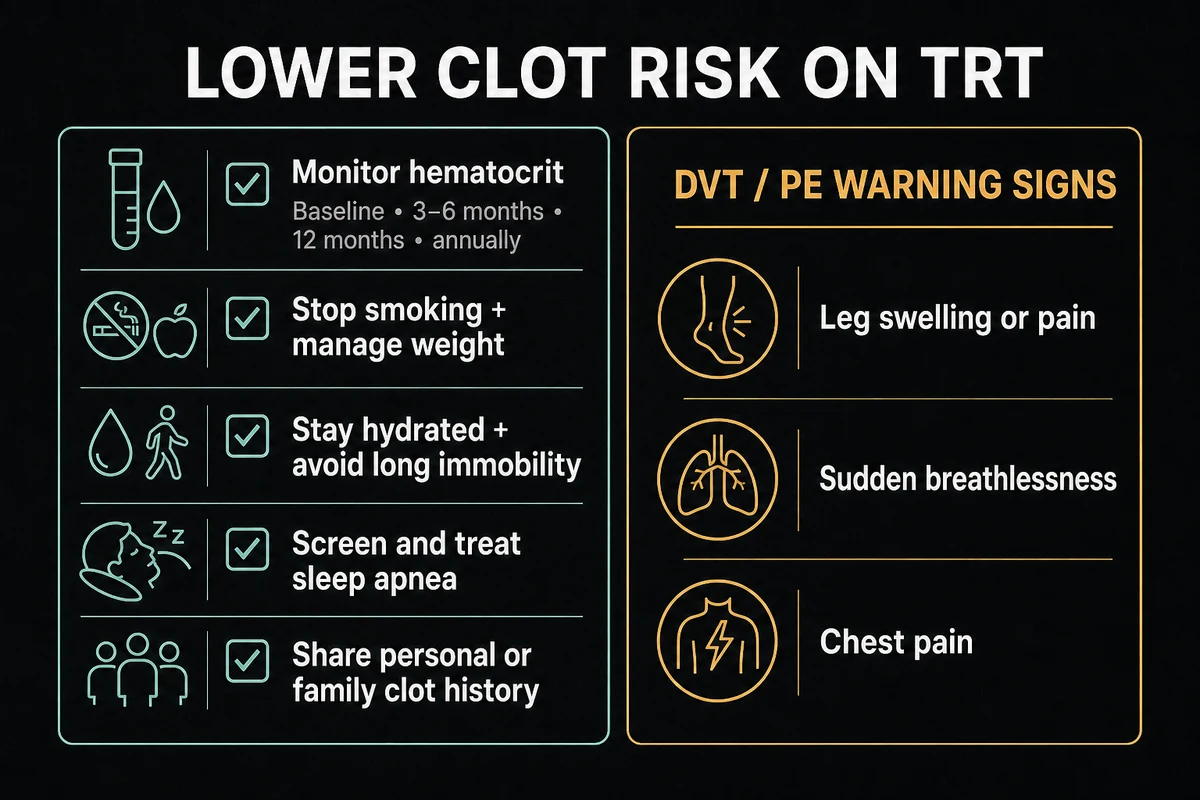
It helps to define the two clots the warning is about. A deep vein thrombosis is a clot that forms in a deep vein, usually in the leg, and a pulmonary embolism is what happens when part of that clot breaks off and travels to the lungs 12. The CDC lists the warning signs worth knowing: for a DVT, swelling, pain, tenderness, or redness in one leg, and for a PE, sudden shortness of breath, chest pain that worsens with a deep breath, a fast heartbeat, or coughing up blood 12. These are the symptoms that warrant urgent medical attention rather than a wait-and-see approach.
Now the absolute-risk framing that the scare blogs skip. Most men on well-monitored TRT do not get a clot. In TRAVERSE, venous thromboembolism occurred in about 1.7% of men on testosterone versus 1.2% on placebo 1. That is a real difference, but it is a modest one, roughly 5 extra events per 1,000 men in that trial, not the blanket danger some vein-clinic pages imply. The clot risk is a modest relative increase, concentrated early, layered on a baseline that is low for most men. That is a very different message from "TRT causes clots" full stop, and it is why clots on TRT belong in the TRT side effects conversation as something to monitor rather than something to fear outright.
Why does TRT raise clot risk? Hematocrit and thick blood
Understanding why matters, because the mechanism tells you exactly what your clinician will manage. Testosterone does not clot your blood by acting on the clotting proteins directly. The dominant pathway runs through red blood cells. Testosterone stimulates erythropoietin (the hormone that tells your bone marrow to make red cells) and suppresses hepcidin (a hormone that regulates iron), and the result is more red blood cells 11. More red cells raise your hematocrit, and a higher hematocrit means thicker, more viscous blood that moves more slowly, which is what raises clot risk 11. Cleveland Clinic frames the same chain plainly: too many red blood cells thicken the blood (hyperviscosity), which raises the risk of clots and stroke 9.
This is why hematocrit is the number that matters, and why a complete blood count is part of standard TRT monitoring. Route and dose change how hard testosterone pushes on this system. Injectable testosterone esters tend to raise hematocrit more than transdermal gels or creams, largely because of the higher peak levels they produce, which is one reason your delivery method is part of the clot conversation and is covered in our guide to TRT dosage 11. The rise is not immediate, hematocrit typically peaks around 8 to 16 weeks after a dose is started or increased, which also happens to be the window when short-term clot risk appears highest 11. The table below ties specific hematocrit levels to the actions guidelines recommend.
Table 1. Hematocrit levels on TRT and what they mean
| Hematocrit | Interpretation | Typical physician action |
|---|---|---|
| 41 to 53% | Normal adult male range | Routine periodic monitoring 311 |
| Above 48% at baseline | Endocrine Society: generally do not start TRT until addressed | Investigate the cause, defer or optimize before starting 3 |
| Around 52% | Watch closely | Recheck, address confounders such as dehydration or sleep apnea 11 |
| Above 54% | Recognized action point | Reduce dose, change route, pause, or arrange therapeutic phlebotomy 34 |
| Above 56% | Urgent | Prompt evaluation, hold therapy, therapeutic phlebotomy 11 |
The recurring 48% and 54% figures come from the Endocrine Society Clinical Practice Guideline and the AUA Testosterone Deficiency Guideline, which is why reputable sources keep landing on the same thresholds 34. Because raised hematocrit also drives blood pressure through the same thicker-blood mechanism, it is the shared engine behind two of the biggest TRT-safety questions, as we cover in TRT and blood pressure.
What TRAVERSE and the research actually show
For years the honest answer to "is TRT good for your heart" was "we do not have a large randomized trial." That changed with TRAVERSE, published in 2023, the first big randomized cardiovascular-safety study of testosterone. It enrolled 5,246 middle-aged and older men who had hypogonadism and either existing cardiovascular disease or a high risk of it, and it asked a direct question: does testosterone raise the rate of major adverse cardiac events (heart attack, stroke, or cardiovascular death)? The answer was no. Major adverse cardiac events occurred in 7.0% of the testosterone group versus 7.3% of the placebo group, meeting the trial's bar for non-inferiority 2. Cedars-Sinai summarized the takeaway for a lay audience: testosterone therapy did not increase the risk of heart attack or stroke in the trial population 10.
That is genuinely reassuring on the big endpoints, and it is why the FDA felt able to remove the boxed cardiovascular warning in 2025 1. But TRAVERSE is not a clean bill of health, and pretending otherwise is exactly the whitewash that clinic lead-gen pages fall into. The same trial found higher rates of three things on testosterone: atrial fibrillation (an irregular heart rhythm), pulmonary embolism (a lung clot), and acute kidney injury 2. Those secondary signals are precisely why the FDA, in the same 2025 update, added the new class-wide clot warning even as it dropped the heart-attack boxed warning 1. The one-line honest read: reassuring on heart attacks, strokes, and cardiovascular death, not a free pass on rhythm and clots.
Reconciling "safe" (TRAVERSE) with "2x clot risk" (Walker 2020)
Here is the contradiction almost no competitor page resolves. If TRAVERSE says testosterone is broadly cardiovascular-safe, why do other studies report a doubling of clot risk? The most-cited of those is Walker and colleagues in JAMA Internal Medicine (2020), a case-crossover analysis of 39,622 men. It found that testosterone was associated with roughly a two-fold increase in short-term venous-thromboembolism risk in the six months after starting, and, notably, this held in men both with hypogonadism and without it, with the risk highest in the first one to three months 5.
The two findings are not actually in conflict once you separate the timeline. TRAVERSE measured major cardiac events averaged over years of follow-up and found no long-term increase in heart attacks or strokes 2. Walker captured a transient, front-loaded clot-risk window right after initiation 5. Put together, the accepted synthesis is this: there is a real but temporary early clot-risk window, front-loaded to roughly the first three to six months, layered on top of neutral long-term cardiac risk. That is why the first few months on TRT deserve the closest attention, and it is also why some men and clinicians consider gentler-on-blood-count alternatives during that window, an idea we return to below.
Does TRT raise cholesterol?
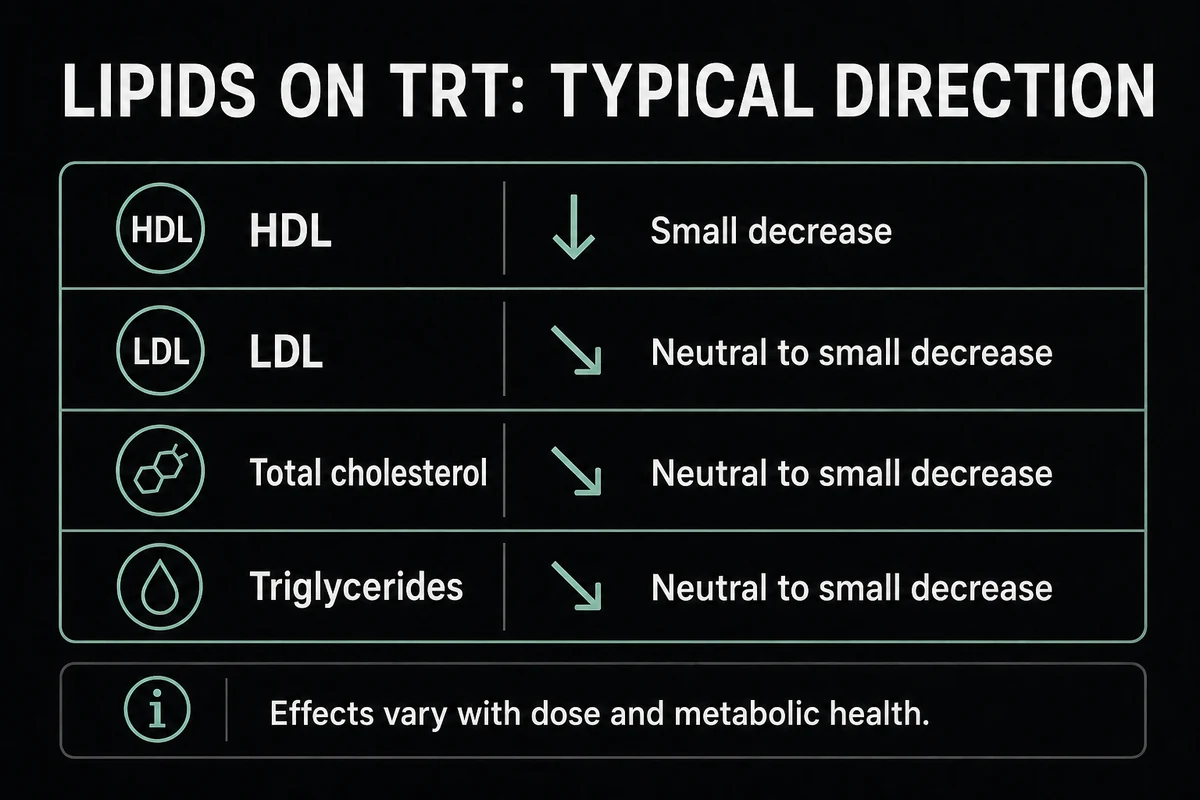
Does TRT raise cholesterol? At the physiologic doses used for replacement, the answer is usually no in any dramatic sense, the lipid changes are modest. The best evidence here is a meta-analysis by Whitsel and colleagues of intramuscular testosterone esters in hypogonadal men, which found a small, dose-dependent decrease in HDL (the "good") cholesterol, alongside concurrent declines in total and LDL (the "bad") cholesterol 8. In other words, testosterone tends to nudge several lipid numbers down at once, which nets out as broadly neutral to mildly favorable for most men on replacement doses, not the cholesterol catastrophe the internet sometimes describes.
Table 2. How TRT affects your cholesterol (physiologic doses)
| Lipid marker | Typical direction on TRT | Notes |
|---|---|---|
| HDL ("good") cholesterol | Small decrease (dose-dependent) | Larger doses tend to lower HDL more 8 |
| LDL ("bad") cholesterol | Neutral to small decrease | Often declines modestly 8 |
| Total cholesterol | Neutral to small decrease | Modest downward shift reported 8 |
| Triglycerides | Neutral to small decrease | Varies with body composition and metabolic health 8 |
The crucial caveat is dose. Everything above describes physiologic replacement. The sharp HDL crash people have read about comes from supraphysiologic anabolic-steroid abuse, doses many times higher than replacement, which is a fundamentally different exposure, as we explain in is TRT a steroid. Do not let bodybuilding-forum horror stories set your expectations for a monitored replacement dose.
Does TRT lower cholesterol?
Because TRT can nudge several lipid markers down, some men ask the opposite question: does TRT lower cholesterol, and could it be used as a cholesterol treatment? The honest reconciliation is that in hypogonadal men, TRT can modestly lower total and LDL cholesterol and triglycerides, partly as body composition, waist size, and insulin sensitivity improve over months 8. But it also tends to pull HDL down, so the picture is mixed, not a uniform improvement. The bottom line: TRT is not a cholesterol therapy. If it moves your lipids in a good direction, treat that as a welcome side effect, not the reason to be on it, and never start or stay on testosterone as a way to manage high cholesterol.
How to lower cholesterol on TRT
If your lipids do run high while on treatment, the approach to how to lower cholesterol on TRT is the same physician-directed, evidence-based care anyone with high cholesterol gets, layered on top of your TRT plan. That means a standard heart-healthy diet, regular aerobic exercise, weight and waist management, and moderating alcohol, plus a review of your testosterone dose and route with your prescriber and keeping estradiol in a sensible range 8. If diet and lifestyle are not enough, lipid-lowering medication such as a statin is added when clinically indicated, exactly as it would be for a man not on TRT. The key YMYL point: your cholesterol is one input among many, and adjusting a statin, your TRT dose, or an aromatase inhibitor is a clinician's call informed by your labs, not a self-managed protocol.
Does TRT increase heart rate and cause palpitations?
Does TRT increase heart rate? For some men there is a modest effect, often just a few beats per minute if any, and it is best understood in absolute terms rather than as an alarm. The plausible mechanisms are indirect: a higher blood volume and hematocrit and some increase in sympathetic (fight-or-flight) tone can nudge resting heart rate up in certain men 11. Many men notice no change at all in their resting heart rate. There is no evidence that replacement-dose testosterone reliably drives a large, dangerous rise in heart rate on its own.
Palpitations, the feeling of a racing, pounding, or skipped heartbeat, have several possible sources on TRT, and it is worth naming them honestly. One is the atrial-fibrillation signal seen in TRAVERSE, since an irregular rhythm can feel like palpitations 2. Others are swings in estradiol, ordinary anxiety, caffeine, poor sleep, or causes entirely unrelated to testosterone. On that last point, "TRT panic attacks" is a common search, and the honest answer is that anxiety and panic symptoms are usually multifactorial rather than a direct testosterone effect, though hormonal changes can be one contributor worth discussing with your clinician. What is not optional is knowing when a rhythm symptom needs urgent care: fainting or near-fainting, chest pain, a sustained racing or irregular pulse, or breathlessness all warrant prompt medical attention rather than waiting it out.
Does TRT enlarge your heart or cause heart failure?
Does TRT enlarge your heart? At replacement doses, the evidence does not show that physiologic TRT causes pathologic heart enlargement. The association between testosterone and thickened heart muscle, left-ventricular hypertrophy, or cardiomyopathy comes overwhelmingly from supraphysiologic anabolic-steroid abuse, the very high doses used for physique and performance, not from prescribed replacement, a distinction we draw out in is TRT a steroid 9. Conflating the two is one of the most common errors in this topic.
Heart failure deserves its own note, because it flips the direction of caution. Rather than TRT reliably causing heart failure, the guidance is that uncontrolled or severe heart failure is a reason to defer or avoid TRT, because adding fluid retention and a higher blood volume to a struggling heart is a bad combination. Both the Endocrine Society guideline and Cleveland Clinic list uncontrolled heart failure among the situations that call for caution or deferral, alongside a recent cardiovascular event 39. If you have significant heart disease, TRT is a decision made carefully with your cardiologist in the loop, not a routine prescription.
How to prevent blood clots on TRT
There is no way to reduce clot risk to zero, but there is a clear, physician-directed set of moves that keeps it low, and none of them is a self-dosing instruction. Learning how to prevent blood clots on TRT starts with monitoring the hematocrit on schedule so thickening is caught early, then controlling the modifiable risks that stack on top of testosterone, and knowing the warning signs so a clot is treated fast if it happens. The table below frames these as clinician-guided steps.
Table 3. How to lower your clot risk on TRT (physician-directed)
| Step | How it helps | Notes |
|---|---|---|
| Monitor hematocrit on schedule | Catches blood thickening before it reaches an action threshold | Baseline, 3 to 6 months, 12 months, then annually 34 |
| Keep hematocrit in range | Lowers blood viscosity, the main clot lever | Via dose or route change, or therapeutic phlebotomy, all clinician-directed 311 |
| Stop smoking and manage weight | Removes additive, independent clot risk factors | Smoking and obesity raise clot risk on their own 12 |
| Stay hydrated and avoid long immobility | Reduces blood stasis that lets clots form | Move on long flights or drives, hydrate well 12 |
| Screen and treat sleep apnea | Untreated apnea drives both hematocrit and blood pressure up | Doubly useful, it sits at the intersection of both risks 11 |
| Disclose clot and thrombophilia history | Informs whether TRT is right for you and how closely to watch | Share personal or family clot history before starting 3 |
| Know DVT and PE warning signs | Turns a dangerous clot into a treated one | Leg swelling or pain, sudden breathlessness, chest pain 12 |
Two of these deserve emphasis. First, disclose any personal or family history of blood clots or a clotting disorder (thrombophilia) before you start, because that history changes both your candidacy and your monitoring intensity, and the Endocrine Society specifically flags thrombophilia as a caution 3. Second, timing TRT after a heart attack or other cardiac event is a coordinated decision with cardiology, since TRAVERSE excluded men with very recent cardiovascular events, so its reassurance does not automatically extend to the immediate aftermath of one 2. Everything in this table is a clinician's decision made from your labs and history, not a checklist to run on your own.
Monitoring your heart on TRT
Monitoring is the safety feature that makes the risks on this page manageable rather than scary. Following the Endocrine Society Clinical Practice Guideline, clinicians measure testosterone and a baseline hematocrit before starting, and they generally do not initiate TRT if baseline hematocrit is above 48% 3. After starting, testosterone and hematocrit are typically rechecked at about 3 to 6 months and at 12 months, then annually once stable, with the guideline advising evaluation and a dose reduction or pause if hematocrit climbs above 54% 3. The AUA guideline similarly calls for measuring hemoglobin and hematocrit at baseline and on follow-up, counseling on the erythrocytosis and thrombotic risk, and discussing cardiovascular risk before initiation 4. Periodic lipid panels and blood-pressure checks round out the cardiovascular picture. Our guide to testosterone levels on TRT covers what these labs mean and how often they are drawn.
A reassuring backstop: because the raised red-cell count is driven by the testosterone itself, hematocrit typically normalizes over roughly 3 to 6 months after therapy is stopped, which is one of the things covered in our page on stopping TRT 3. And for men worried specifically about the hematocrit-and-clot mechanism, it is worth knowing that not every route to higher testosterone drives red cells the same way. Medications that raise your body's own testosterone production, rather than adding external hormone, tend to cause less of a hematocrit spike, one reason some men and clinicians discuss options such as those covered in our enclomiphene guide. That is a different tool for a different goal, and still a prescription decision, but it is a legitimate part of the conversation when clot risk is the concern.
Frequently Asked Questions
For some men, yes, mainly in the first few months and mainly because testosterone raises the red blood cell count and thickens the blood. Every testosterone product now carries an FDA class-wide venous-thromboembolism warning added in February 2025, and in the TRAVERSE trial clots occurred in about 1.7% of men on testosterone versus 1.2% on placebo 12. The risk is real but modest in absolute terms and is managed with hematocrit monitoring.
You cannot make the risk zero, but you can keep it low with physician-directed steps: monitor hematocrit on schedule, keep it in range through dose or route changes or phlebotomy, stop smoking, manage weight, stay hydrated, avoid long immobility, treat sleep apnea, and disclose any personal or family clot history before starting 31112. Knowing the warning signs of DVT and PE means a clot gets treated fast if it does happen 12.
At physiologic replacement doses, not much. Testosterone tends to cause a small, dose-dependent drop in HDL cholesterol alongside neutral-to-lower total and LDL cholesterol, which nets out as broadly neutral to mildly favorable for most men 8. The dramatic HDL crashes people read about come from supraphysiologic anabolic-steroid abuse, not from monitored replacement.
It can, modestly, often just a few beats per minute if at all, through a higher blood volume and hematocrit and some sympathetic-tone effect, and many men notice no change 11. There is no evidence that replacement-dose testosterone reliably causes a large or dangerous rise in resting heart rate on its own.
Palpitations on TRT can have several sources, including the atrial-fibrillation signal seen in TRAVERSE, swings in estradiol, anxiety, caffeine, or causes unrelated to testosterone 2. Fainting, chest pain, a sustained racing or irregular pulse, or breathlessness warrant prompt medical attention rather than waiting.
The large TRAVERSE trial found no increase in heart attacks, strokes, or cardiovascular deaths on testosterone (major adverse cardiac events were 7.0% versus 7.3% on placebo), which is why the FDA removed the boxed cardiovascular warning in 2025 12. The same trial did record more atrial fibrillation, pulmonary embolism, and acute kidney injury, so testosterone is reassuring on heart attacks but not a clean pass on rhythm and clots 2.
References
- U.S. Food and Drug Administration. FDA issues class-wide labeling changes for testosterone products. February 2025.
- Lincoff AM, Bhasin S, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023;389(2):107-117.
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline (2018, validity confirmed 2024).
- Walker RF, et al. Association of Testosterone Therapy With Risk of Venous Thromboembolism Among Men With and Without Hypogonadism. JAMA Intern Med. 2020;180(2):190-197.
- Harvard Health Publishing. FDA warns about blood clot risk with testosterone products. 2014.
- MedlinePlus. Testosterone Injection. U.S. National Library of Medicine. Accessed 2026.
- Whitsel EA, et al. Intramuscular testosterone esters and plasma lipids in hypogonadal men: a meta-analysis. Am J Med. 2001;111(4):261-269.
- Cleveland Clinic. Testosterone Replacement Therapy (TRT). Accessed 2026.
- Cedars-Sinai. Research Finds Testosterone Therapy Safe for Heart Health. Accessed 2026.
- Ohlander SJ, et al. Erythrocytosis Following Testosterone Therapy. Sex Med Rev. 2018;6(1):77-85 (PMC5647167).
- Centers for Disease Control and Prevention. About Blood Clots. Accessed 2026.
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.