
Does TRT raise blood pressure? For some men, yes, and the honest, guideline-anchored answer is that testosterone can modestly raise blood pressure, mainly by increasing your red blood cell count (hematocrit) and thickening your blood, with a smaller push from mild fluid retention. The effect is variable, not every man's blood pressure climbs, and the rise is often modest, but it is real enough that in February 2025 the U.S. Food and Drug Administration added a class-wide blood-pressure warning to every testosterone product after ambulatory blood-pressure-monitoring studies confirmed an increase 1. The important part: this is monitorable and manageable, not usually a reason to avoid testosterone replacement therapy if your blood pressure is controlled and tracked. This page fuses the two questions most articles split, the yes/no safety question and the hematocrit plus blood-donation management job, with real thresholds and resolvable citations.
Key Takeaways
- Yes, but usually modest: TRT can raise blood pressure in some men, the effect is variable, and it is manageable with monitoring rather than a reason to rule out treatment for most people with controlled BP 15.
- The FDA added a class-wide BP warning in 2025: after ambulatory blood-pressure-monitoring data, every testosterone product now carries a blood-pressure warning, while the older boxed cardiovascular warning was removed 1.
- Hematocrit is the main driver: testosterone stimulates red blood cell production, which raises hematocrit and blood thickness (viscosity), and that is why the blood-pressure and blood-count conversations are the same conversation 711.
- 54% is the recognized action threshold: guidelines flag a hematocrit above roughly 54% as a point to act (reduce dose, change route, pause, or arrange a blood draw), and they advise not starting TRT if baseline hematocrit is above 48% 23.
- Blood donation and phlebotomy are physician-directed: whole-blood donation is allowed at most every 56 days, but frequency should be driven by your labs, and therapeutic phlebotomy is a prescribed medical draw, not a hobby 1012.
- Control blood pressure before you start: uncontrolled hypertension is a reason to optimize first, not usually an absolute barrier, and both BP and hematocrit are checked at baseline and on a schedule afterward 28.
Does TRT raise blood pressure?
Yes, testosterone replacement therapy can raise blood pressure in some men, and the strongest signal for this is now written directly into the drug labels. In February 2025 the FDA issued class-wide labeling changes for testosterone products, adding a warning that these products can increase blood pressure after ambulatory blood-pressure-monitoring (ABPM) studies confirmed a class-wide rise 1. That same update removed the older boxed cardiovascular-outcomes warning and incorporated results from the large TRAVERSE trial, so the net message is nuanced: the feared heart-attack and stroke signal was not confirmed, while a blood-pressure caution was added 14.
The patient-facing drug information says the same thing in plainer language. MedlinePlus notes that testosterone may cause an increase in blood pressure and lists a raised risk of heart attack or stroke among the reasons for careful use 5. The topical label carries the matching class blood-pressure caution 6.
What the labels do not say is that every man will see a jump. The effect is variable and often modest. Many men on well-monitored TRT see little or no change in their readings, while others, especially on higher or injectable doses that push red blood cell counts up, see a measurable rise. That variability is exactly why the guidance is to monitor rather than to assume, and it is why "does TRT cause high blood pressure" has no single yes-or-no answer that fits everyone.
Why does TRT raise blood pressure?
Understanding why does TRT raise blood pressure matters, because the mechanism tells you what to manage. Testosterone does not mainly work by pushing directly on your artery walls. The dominant pathway is indirect and runs through your blood itself, with a smaller contribution from fluid balance and estrogen.
High hematocrit on TRT and thicker blood
The main driver is erythropoiesis, the production of red blood cells. Testosterone stimulates your body to make more red blood cells, which raises your hematocrit (the percentage of your blood made up of red cells) and, with it, your blood's thickness or viscosity 711. Thicker blood is harder to move, which can nudge blood pressure up and, at the extreme, raise clot risk. This is the same effect people describe as high hematocrit on TRT or "trt thick blood," and it is the reason a complete blood count is part of standard monitoring.
Route matters here. Injectable testosterone esters tend to raise hematocrit more than transdermal gels or creams, largely because of the higher peak levels they produce 12. That is why men on injections may need closer blood monitoring than men on a daily gel, and why your choice of formulation is part of the blood-pressure conversation. Our guide to types of TRT compares how the delivery methods differ, and TRT dosage covers how dose and injection frequency change those peaks.
Fluid retention, estrogen, and blood pressure
The second pathway is fluid. Testosterone can cause mild sodium and water retention, especially in the first weeks, and holding onto extra fluid can raise blood pressure modestly 57. Some of testosterone is also converted to estradiol (a form of estrogen) by an enzyme called aromatase, and estrogen influences fluid balance too, which is why some men ask about high estrogen and high blood pressure on TRT. This is a real but usually secondary contributor compared with the red-cell mechanism.
The key YMYL point: managing estrogen is a physician-directed decision, not a do-it-yourself project. Aromatase-inhibitor medicines are prescription drugs used carefully and only when indicated, and driving estrogen too low creates its own problems (joint pain, low libido, mood and bone effects). If your clinician thinks estradiol is contributing, that is a lab-guided adjustment, not something to chase from a forum protocol.
Can TRT lower blood pressure?
You will find claims online that TRT lowers blood pressure, and honesty requires reconciling them rather than pretending they do not exist. Some older observational and metabolic studies in men with genuinely low testosterone reported reductions in blood pressure or pulse pressure as those men lost fat, gained muscle, and improved their insulin sensitivity over time. In that specific setting, treating a real deficiency and improving overall metabolic health can move numbers in a good direction indirectly.
That does not overturn the current label position. The controlled ambulatory blood-pressure-monitoring data that drove the 2025 FDA update showed that testosterone products, as a class, increase blood pressure 1. The right way to hold both facts at once: improving low testosterone and body composition may help some men's cardiovascular risk profile, but testosterone itself is not a blood-pressure treatment, and you should never start or continue TRT as a way to manage hypertension. If your blood pressure is high, it needs its own diagnosis and its own management, guided by your clinician.
What is normal blood pressure on TRT?
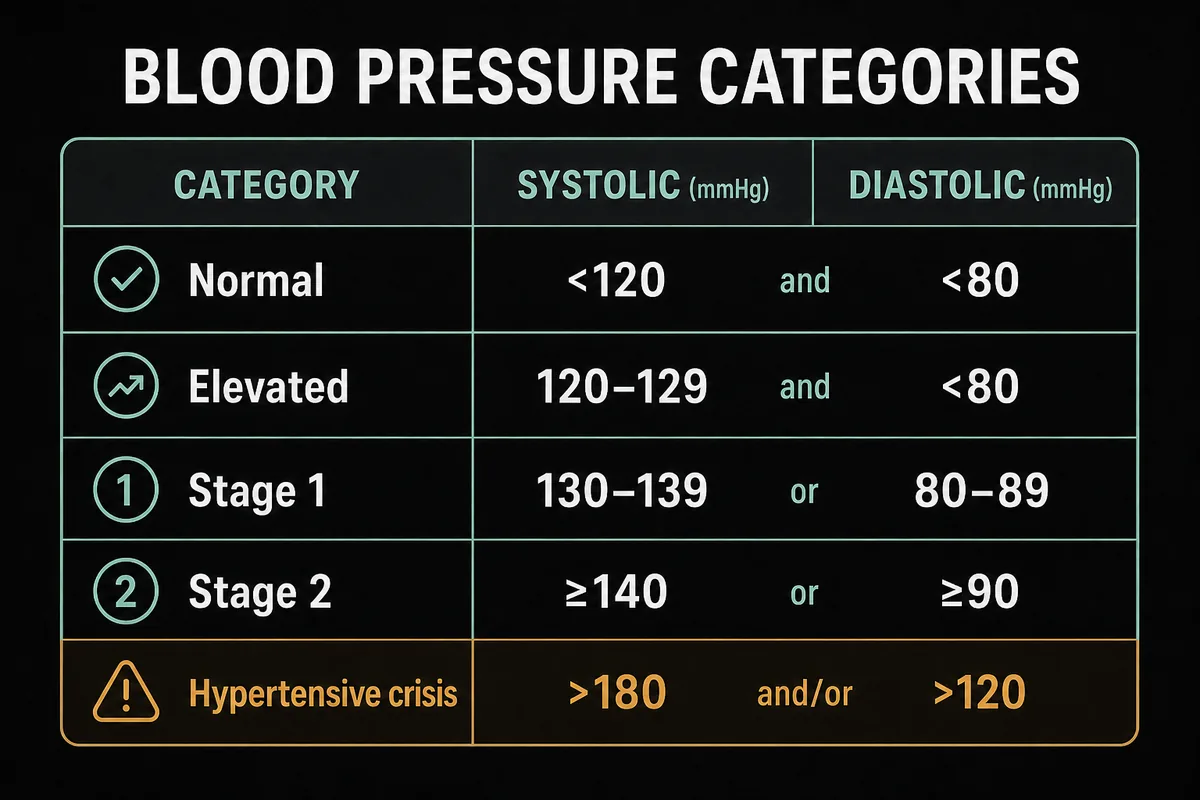
There is nothing special about the target for a man on testosterone. Normal blood pressure on TRT is the same as normal blood pressure for anyone, using the American Heart Association categories below. The goal is a controlled reading with periodic home monitoring, and a single high reading is not a diagnosis; blood pressure is diagnosed on a pattern of readings, not one bad afternoon.
Table 1. Blood pressure categories (American Heart Association)
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | Less than 120 | and less than 80 |
| Elevated | 120 to 129 | and less than 80 |
| Stage 1 hypertension | 130 to 139 | or 80 to 89 |
| Stage 2 hypertension | 140 or higher | or 90 or higher |
| Hypertensive crisis | Higher than 180 | and/or higher than 120 |
A hypertensive-crisis reading (roughly above 180 over 120) with symptoms such as chest pain, shortness of breath, or vision changes is a medical emergency, not a wait-and-see. For everyday tracking, a validated home cuff, taken while seated and rested, is the practical tool your clinician will want you to use.
Can you take TRT with high blood pressure?
For most men, high blood pressure is not an absolute barrier to TRT, but it changes the order of operations. Can you take TRT with high blood pressure? Usually yes, if the blood pressure is controlled first and then monitored during treatment. Uncontrolled hypertension is a reason to optimize before starting, not necessarily forever, and your clinician will typically want your readings in a reasonable range before adding a therapy that can nudge them up 18.
That said, some situations do call for holding off or extra caution. Guideline and clinic sources flag conditions such as a very high baseline red blood cell count (hematocrit above about 54%), uncontrolled heart failure, and a recent cardiovascular event as reasons to defer or avoid TRT until the picture is safer 238. This is exactly the ground your clinician covers before writing a prescription, alongside the pre-treatment labs described below. If you already take blood-pressure medication, that is worth raising early, because it becomes part of the monitoring plan rather than a disqualifier.
High hematocrit on TRT: symptoms and safe levels
Because raised hematocrit is the engine behind the blood-pressure effect, it deserves its own numbers. High hematocrit on TRT (sometimes called polycythemia or, more precisely, secondary erythrocytosis) is the single most consistent lab change on testosterone, and it typically peaks around 8 to 16 weeks after a dose is started or increased 1112. Many men have no symptoms at all and it is caught only on bloodwork, which is the whole argument for routine monitoring.
When high hematocrit symptoms on TRT do appear, they can include headaches, facial flushing or redness, dizziness, and fatigue, and in rare cases the real concern is a clot from thicker, slower-moving blood 711. A useful nuance: iron deficiency can mask a high hematocrit by keeping hemoglobin looking "normal," so your clinician may look at the full picture rather than one number 11. The table below ties specific hematocrit levels to the actions guidelines recommend.
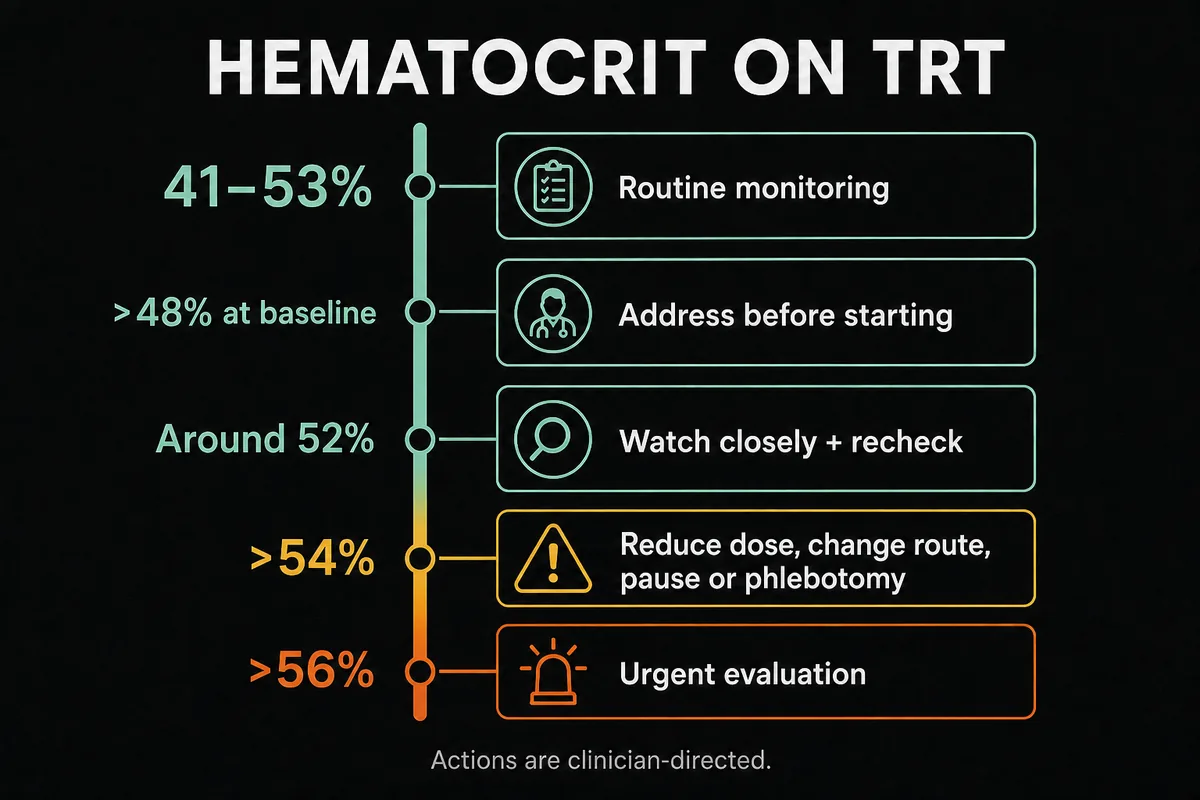
Table 2. Hematocrit levels on TRT and what they mean
| Hematocrit | Interpretation | Typical physician action |
|---|---|---|
| 41 to 53% | Normal adult male range | Routine periodic monitoring 211 |
| Above 48% at baseline | Endocrine Society: generally do not start TRT until addressed | Investigate the cause, defer or optimize before starting 2 |
| Around 52% | Watch closely | Recheck, address confounders, consider phlebotomy 12 |
| Above 54% | Recognized action point | Reduce dose, change route, pause, or arrange therapeutic phlebotomy 23 |
| Above 56% | Urgent | Prompt evaluation, hold therapy, therapeutic phlebotomy 1112 |
These thresholds come from the Endocrine Society Clinical Practice Guideline and the AUA Testosterone Deficiency Guideline, which is why the 54% figure recurs across reputable sources 23. Hematocrit is also a recurring theme in our broader guide to TRT side effects, where polycythemia and blood pressure both appear.
How to lower hematocrit on TRT
If your hematocrit climbs, there is a clear, evidence-ordered set of moves, and the first one is rarely the dramatic one. Knowing how to lower hematocrit on TRT starts with fixing the confounders (dehydration, untreated sleep apnea, high altitude, and smoking all push red cells up on their own), then adjusting how the testosterone is delivered, and only then reaching for blood removal or dose cuts 1112. Every step below is a clinician's decision made from your labs, not a self-management checklist.
Table 3. Ways to lower hematocrit and blood pressure on TRT (physician-directed)
| Strategy | How it helps | Notes |
|---|---|---|
| Fix confounders | Removes non-TRT drivers of high red cell counts | Hydration, sleep-apnea treatment, altitude, and smoking cessation 11 |
| Split injection frequency | Lowers the peak levels that drive erythropoiesis | Smaller, more frequent doses smooth the peaks 12 |
| Switch injectable to gel or cream | Transdermal routes raise hematocrit less than injections | A common step when counts run high 12 |
| Whole blood donation | Physically removes red cells, lowering hematocrit | Allowed at most every 56 days; eligibility-gated 10 |
| Therapeutic phlebotomy | Prescribed blood draw to reduce red cell mass | Ordered by a clinician; not a fixed schedule 12 |
| Dose reduction | Lowers the erythropoietic drive at the source | Usually not the first move; balanced against symptom control 2 |
| Pause or stop TRT | Removes the driver entirely | Last resort; hematocrit normalizes over about 3 to 6 months 2 |
Dose reduction is usually not the first lever, because it can bring back the low-testosterone symptoms you were treating. More often, splitting the injection frequency or moving to a transdermal route handles a rising count without giving up the benefits, which is one reason TRT injection sites and technique come up in these conversations.
Donating blood on TRT: how often should you donate
Blood donation is the tool most men reach for, and it works because it physically removes red cells. How often should you donate blood on TRT? The ceiling for whole-blood donation is set by the American Red Cross at most every 56 days (8 weeks), and that is a safety limit for everyone, not a TRT prescription 10. The right frequency for you is driven by your lab results, not by a fixed calendar, so some men never need to donate and others need periodic draws timed to their hematocrit.
A practical note on eligibility: donation centers screen donors, and being on TRT does not automatically disqualify you, but you should answer their questions honestly. If donation is being used specifically to manage a medical high hematocrit, that is really the territory of therapeutic phlebotomy, described next.
Blood donation vs therapeutic phlebotomy
These two look similar (both remove a unit of blood) but they are different processes. Voluntary blood donation is free, eligibility-gated, and altruistic; the blood goes to patients, and you have to meet donor criteria. Therapeutic phlebotomy is a prescribed medical draw ordered by a clinician for a diagnosis such as erythrocytosis, usually documented with a script and an ICD-10 code, and it can be done even when standard donor eligibility rules would otherwise turn you away 12. Men sometimes ask whether donating plasma helps; plasma donation does not remove red cells, so it does not lower hematocrit even though it is generally allowed.
What happens if you don't donate blood on TRT
Donating blood is not a mandatory part of TRT, and it is worth stating plainly because the folk wisdom online often implies it is. What happens if you don't donate blood on TRT depends entirely on your hematocrit. If your counts stay in the normal range, you may never need a draw at all. Blood removal is only needed when hematocrit climbs toward the action thresholds in Table 2 23. The risk of ignoring a genuinely high, sustained hematocrit is that thicker blood raises viscosity and clot risk over time, which is precisely why monitoring exists, so the number, not a habit, drives the decision.
Protecting your iron after repeated draws
There is a trap on the other side. Repeated blood removal depletes iron, and over-phlebotomy can drop your ferritin (stored iron) low enough to cause fatigue and, paradoxically, can drive a reactive rebound in red-cell production 1112. This is why frequent draws are not a "more is better" strategy and why your clinician may check ferritin, not just hematocrit. The aim is the least blood removal that keeps your count safe, balanced against your iron stores, which again is a physician-directed calculation rather than a self-managed routine.
How to lower blood pressure on TRT
Managing blood pressure on TRT layers standard hypertension care on top of getting the hematocrit right. In practice, how to lower blood pressure on TRT starts with controlling the red-cell mechanism first (the steps in Table 3), because thick blood is often the specific TRT-related contributor. From there, the levers are the same ones that work for anyone: reducing sodium, losing excess weight, regular aerobic exercise, moderating alcohol, and improving sleep 7. Screening for and treating obstructive sleep apnea is doubly useful here, because untreated apnea raises both hematocrit and blood pressure, so it sits at the intersection of the two problems.
If lifestyle measures are not enough, antihypertensive medication is added when indicated, exactly as it would be for a man not on TRT, and your clinician may also review your estradiol and your testosterone dose or route as part of the picture 18. The through-line is that this is coordinated care: your blood-pressure management and your TRT are tuned together, not in separate silos. Our companion page on TRT and heart health covers the broader cardiovascular context, including what the TRAVERSE trial did and did not show (it found no rise in major cardiac events but did note higher rates of atrial fibrillation and pulmonary embolism) 49.
Monitoring blood pressure and hematocrit on TRT
Monitoring is the safety feature that turns a list of risks into manageable ones. Following the Endocrine Society Clinical Practice Guideline, clinicians check blood pressure and a baseline complete blood count (for hematocrit and hemoglobin) before starting, and they generally do not initiate TRT if baseline hematocrit is above 48% 2. After starting, hematocrit is typically rechecked at about 3 to 6 months and then annually once stable, with more frequent checks if a value runs high, and the guideline advises evaluating and reducing or pausing therapy if hematocrit climbs above 54% 23. The AUA guideline similarly calls for measuring hemoglobin and hematocrit at baseline and on follow-up and counseling on polycythemia risk 3.
A common question: will stopping TRT lower hematocrit? Yes. Because the raised red-cell count is driven by the testosterone, hematocrit typically normalizes over roughly 3 to 6 months after therapy is stopped 2. That is a reassuring backstop, but it is not the first-line fix, since stopping also brings back the symptoms you were treating; our page on stopping TRT walks through how a planned pause or discontinuation is handled. Men who want to raise testosterone with less of a hematocrit spike sometimes ask about alternatives; for the fertility-preserving option that stimulates the body's own testosterone rather than adding external hormone, see our enclomiphene guide, which tends to be gentler on blood counts, though it is a different tool for a different goal and is still a prescription decision.
Frequently Asked Questions
It can. Testosterone products carry a class-wide FDA warning, added in February 2025, that they may increase blood pressure, based on ambulatory blood-pressure-monitoring studies 1. The effect is variable and often modest, driven mainly by a rising red blood cell count and mild fluid retention rather than a direct effect on arteries 711. It is monitored and managed rather than assumed.
Usually yes, if the blood pressure is controlled first and then monitored during treatment. Uncontrolled hypertension is a reason to optimize before starting, not typically a permanent barrier, and your clinician will want your readings in a reasonable range and will track both blood pressure and hematocrit on a schedule 18. Certain conditions, such as a very high baseline hematocrit or recent cardiovascular events, call for deferring or avoiding TRT 23.
There is no fixed schedule. Whole-blood donation is allowed at most every 56 days (8 weeks) as a general safety limit, but whether and how often you actually need it should be driven by your hematocrit results, not a calendar 10. Some men never need to donate; others need periodic draws, which if done for a medical high hematocrit are really therapeutic phlebotomy ordered by a clinician 12.
The same as for anyone. Using American Heart Association categories, normal is below 120 over 80, with elevated, stage 1, and stage 2 hypertension defined above that (see Table 1). The goal on TRT is a controlled reading confirmed by home monitoring over time, since a single high reading is not a diagnosis.
Some older observational studies in men with low testosterone reported blood-pressure or pulse-pressure improvements as body composition and metabolic health improved, but this is indirect. The current FDA label position, based on controlled ambulatory data, is that testosterone products increase blood pressure, so TRT should never be used as a treatment for hypertension 1.
Nothing, if your hematocrit stays in the normal range, because donation is not a mandatory part of TRT. Blood removal is only needed when hematocrit climbs toward the action thresholds around 54% 23. The concern with ignoring a genuinely high, sustained hematocrit is that thicker blood raises viscosity and clot risk, which is exactly why the level is monitored and the decision is based on your labs.
References
- U.S. Food and Drug Administration. FDA issues class-wide labeling changes for testosterone products. February 2025.
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline (2018, validity confirmed 2024).
- Lincoff AM, Bhasin S, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023;389(2):107-117.
- MedlinePlus. Testosterone Injection. U.S. National Library of Medicine. Accessed 2026.
- MedlinePlus. Testosterone Topical. U.S. National Library of Medicine. Accessed 2026.
- Mayo Clinic. Testosterone therapy: Potential benefits and risks as you age. Accessed 2026.
- Cleveland Clinic. Testosterone Replacement Therapy (TRT). Accessed 2026.
- Harvard Health Publishing. Testosterone therapy may be safe for men at risk for heart attack and stroke. Accessed 2026.
- American Red Cross. Eligibility requirements for blood donation. Accessed 2026.
- Ohlander SJ, et al. Erythrocytosis Following Testosterone Therapy. Sex Med Rev. 2018;6(1):77-85 (PMC5647167).
- Basheer B, et al. Management of Adverse Effects in Testosterone Replacement Therapy. Int Braz J Urol. 2025 (PMC12052019).
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.