TRT dosage for most men lands in a familiar range: roughly 100 to 200 mg of testosterone cypionate or enanthate per week, usually split into two or more injections and then titrated to your labs and symptoms rather than fixed at one number 123. That single range answers the most common question, but it is only a starting point. Testosterone replacement therapy is a prescription, Schedule III controlled treatment approved for diagnosed hypogonadism, not for aging or performance, and every dose on this page is educational, not a self-dosing protocol 6. Your prescriber sets and adjusts your dose from blood work and how you feel, not from a chart. For the full picture of what the therapy involves, start with our testosterone replacement therapy pillar guide.
Key Takeaways
- Typical range is 100 to 200 mg per week of testosterone cypionate or enanthate, most often split into twice-weekly injections 12.
- Dose is titrated to labs, not to a target number. Clinicians aim for a mid-normal trough total testosterone (often around 450 to 600 ng/dL) that resolves symptoms, not the top of the reference range 12.
- Frequency matters as much as the weekly total. More frequent, smaller injections give a steadier trough and a lower peak, which is why many protocols split the weekly dose 1.
- Microdosing means smaller, more frequent doses, usually daily or every-other-day subcutaneous injections for smoother levels; the evidence base is still limited 7.
- Aromatase inhibitors like anastrozole are not routine. The Endocrine Society and AUA do not recommend routine estrogen blockers, and over-suppressing estradiol harms male bone and libido 129.
- If your dose is too high, the fix is to lower the dose, not to add more drugs; a rising red blood cell count is the classic signal 17.
| Metric | Typical value |
|---|---|
| Typical weekly dose | 100 to 200 mg cypionate or enanthate 12 |
| Common starting dose | 100 to 120 mg/week 12 |
| Most common frequency | Twice weekly |
| FDA-label schedule (older) | 50 to 400 mg every 2 to 4 weeks 312 |
| Target total-T trough | About 450 to 600 ng/dL, individualized 12 |
| First lab recheck | 6 to 8 weeks after a change 12 |
| Hematocrit action threshold | 52 to 54% or higher 7 |
What Is a Normal TRT Dose?
A normal TRT dose in modern practice is the amount of testosterone that restores a genuinely low level back into the normal male range and resolves symptoms, which for injectable testosterone usually means about 100 to 200 mg of cypionate or enanthate per week 12. The goal is physiologic replacement, not maximization: clinicians typically aim for a trough total testosterone somewhere in the mid-normal range, often around 450 to 600 ng/dL, individualized to the person rather than pushed to the top of the reference range 12. A standard TRT dose and a typical TRT dose describe the same thing, the middle of that band, while a normal TRT dosage is defined by where your labs and symptoms land, not by a fixed milligram figure.
This split-dose practice differs from the original FDA label. The Depo-Testosterone (cypionate) prescribing information lists 50 to 400 mg intramuscularly every 2 to 4 weeks, a schedule written decades ago 312. Giving a large dose every few weeks produces a high peak and a low trough, so most clinicians now prescribe smaller amounts more often to keep levels steadier, even though the label language still reflects the older approach 3.
TRT Starting Dose
A common TRT starting dose is 100 to 120 mg of testosterone cypionate or enanthate per week, and some clinicians begin lower, around 80 to 100 mg, especially in older men or those with borderline labs 12. Starting conservatively and rechecking blood work at about 6 to 8 weeks before adjusting is the standard approach, because it takes several weeks for levels to stabilize and for symptoms to respond 12. Your starting TRT dose is a first estimate, not your final dose; the first lab recheck is what tells your clinician whether to hold, raise, or lower it.
TRT Dosage Chart by Delivery Method
There is no single TRT dosage chart that fits every product, because the dose depends heavily on how testosterone is delivered. The table below lines up the common US formulations with typical doses, frequency, and key notes, anchored to FDA labels where available. These are label and clinical-practice ranges, not a personal prescription. For a fuller comparison of each option, see our guide to the types of TRT.
| Method | Typical dose | Frequency | Notes |
|---|---|---|---|
| Testosterone cypionate injection | 100 to 200 mg/week | Once to several times weekly | Most common US injectable ester; IM or subcutaneous 3 |
| Testosterone enanthate injection | 100 to 200 mg/week | Once to several times weekly | Behaves almost identically to cypionate 13 |
| Testosterone gel (AndroGel 1.62%) | Start 40.5 mg/day, range 20.25 to 81 mg/day | Once daily | Transdermal; skin-transfer caution to partners and children 4 |
| Oral testosterone undecanoate (Jatenzo) | Start 237 mg twice daily, titrate 158 to 396 mg twice daily | Twice daily with food | Carries a blood-pressure warning; dose adjusted by labs 5 |
| Subcutaneous pellets (Testopel) | About 150 to 450 mg implanted | Every 3 to 6 months | Steady release but hard to adjust once implanted 12 |
| Compounded testosterone cream | About 50 to 100 mg applied daily | Once or twice daily | Transdermal and compounded, so less standardized than labeled products 12 |
Injectable esters cover most US prescriptions; gels suit men who prefer no needles but require the daily transference precaution, oral undecanoate (Jatenzo) is titrated by labs and carries a blood-pressure warning, and pellets cannot be fine-tuned once implanted 4512.
Testosterone Cypionate TRT Dosage
Testosterone cypionate is the most commonly prescribed injectable ester in the US, and a testosterone cypionate TRT dosage of 100 to 200 mg per week covers most men 3. Cypionate has a long half-life, so a single weekly injection produces a peak in the first few days and a gradual decline to a trough before the next dose 13. That is why a dose like 200 mg per week sits at the upper edge of replacement: given all at once it can push the peak above the normal range even when the trough looks fine, which is one reason splitting it into two 100 mg injections is common 13. Testosterone enanthate behaves almost identically and is dosed the same way. People searching for "trt 200mg per week" or "trt 100mg a week" are describing the two ends of that band, with the right number set by labs, not by preference.
TRT Dosage Per Week and How to Calculate Your Dose (mg to mL)
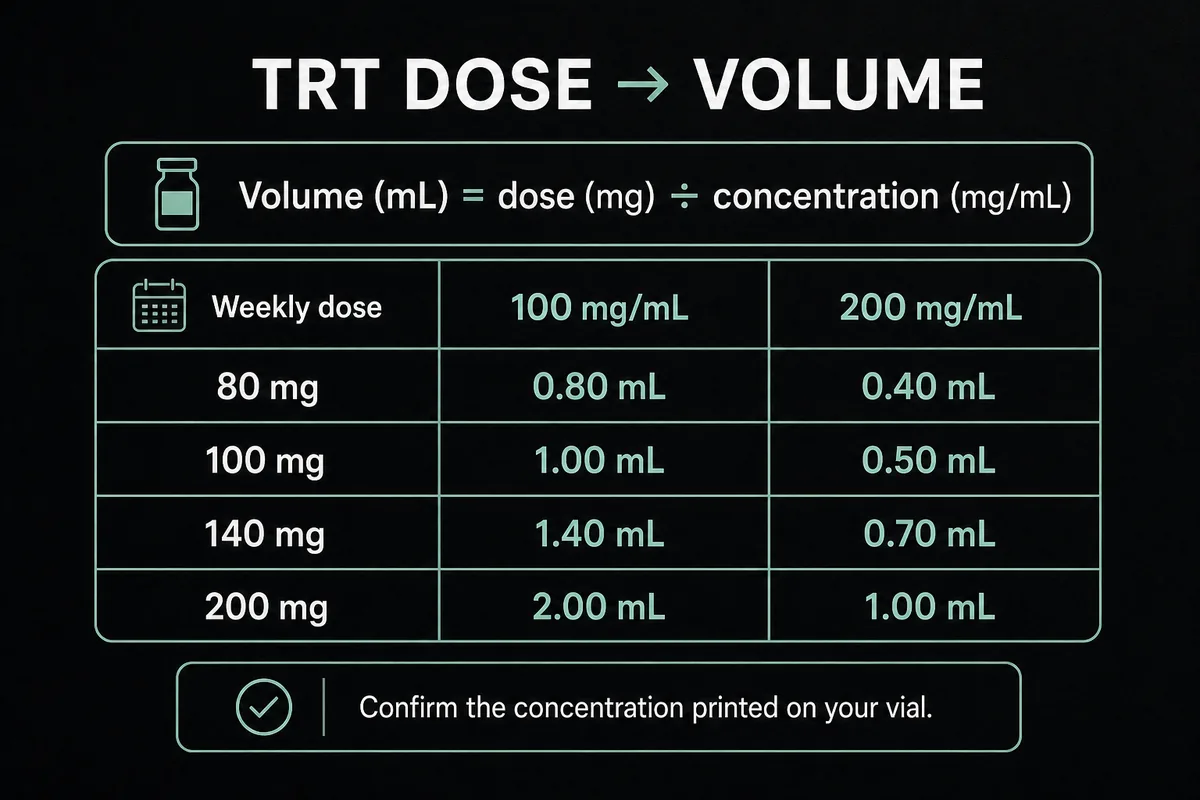
Your TRT dosage per week is a total amount of testosterone, but you inject a volume of liquid, so the practical question is how many milligrams equal how many milliliters. This is the arithmetic behind every "trt calculator" or "trt dosage calculator," shown here transparently rather than hidden in a widget. The conversion depends on the concentration of your vial, which in the US is almost always 100 mg/mL or 200 mg/mL 3.
The formula is simple: volume (mL) equals weekly dose (mg) divided by concentration (mg/mL). A 140 mg weekly dose from a 200 mg/mL vial is 140 divided by 200, or 0.7 mL per week; split into two shots that is 0.35 mL each. The table below does the math for common weekly doses.
| Weekly dose (mg) | Volume at 100 mg/mL | Volume at 200 mg/mL |
|---|---|---|
| 80 mg | 0.80 mL | 0.40 mL |
| 100 mg | 1.00 mL | 0.50 mL |
| 120 mg | 1.20 mL | 0.60 mL |
| 140 mg | 1.40 mL | 0.70 mL |
| 160 mg | 1.60 mL | 0.80 mL |
| 200 mg | 2.00 mL | 1.00 mL |
If you split a weekly dose across multiple injections, divide the weekly volume by the number of shots, and use a syringe graduated finely enough to measure that small per-injection volume accurately. Your prescriber and pharmacist confirm the concentration printed on your specific vial, because reading the wrong concentration (mistaking a 200 mg/mL vial for 100 mg/mL, or the reverse) is the most common dosing error.
TRT Injection Frequency: Twice a Week vs Once a Week vs Daily
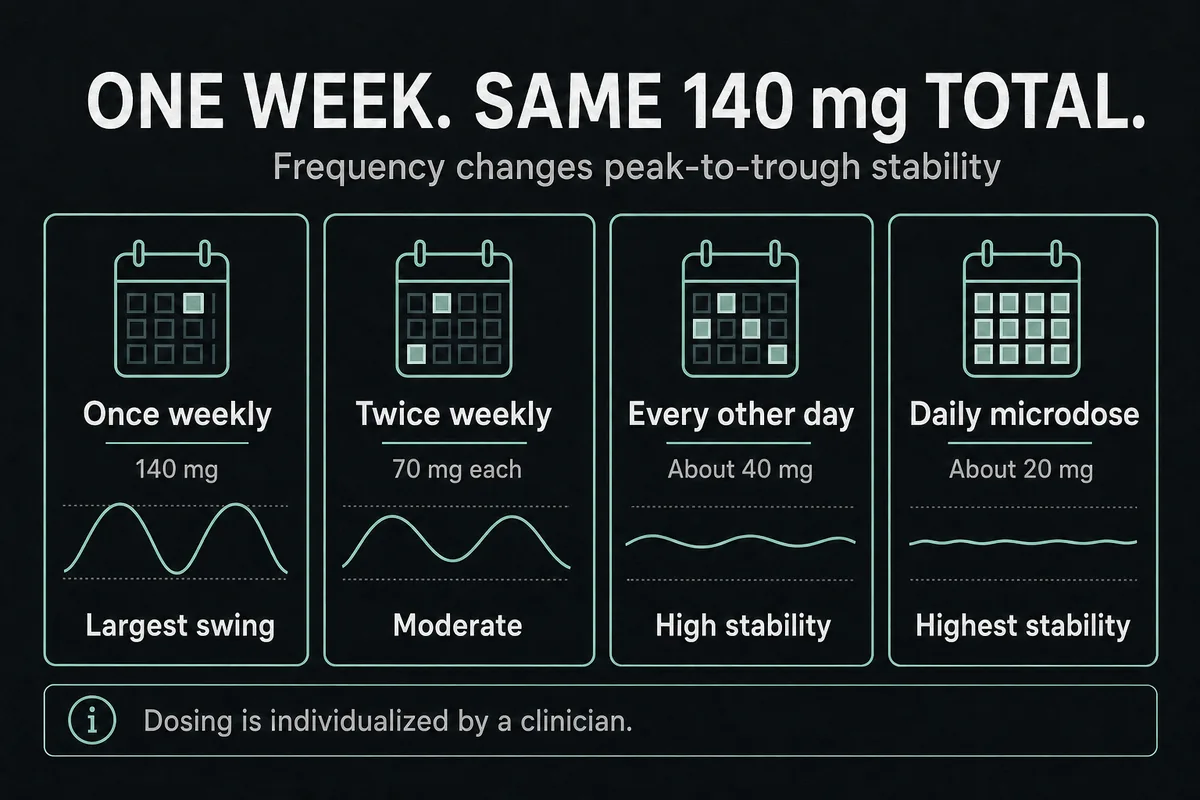
TRT injection frequency changes how steady your levels are, even when the weekly total is identical. Because testosterone cypionate and enanthate have a half-life of roughly 5 to 8 days, a once-weekly injection creates a noticeable peak and trough, while splitting the same weekly amount into smaller, more frequent doses flattens that curve 13. The table uses a 140 mg weekly dose as a worked example.
| Frequency | Per-injection dose | Peak-trough stability | Notes |
|---|---|---|---|
| Once weekly | 140 mg | Largest swing | Simplest schedule, biggest hormone fluctuation |
| Twice weekly | 70 mg | Moderate | The most common clinical split |
| Every other day | About 40 mg | High | Steadier trough, more injections |
| Daily microdose | About 20 mg | Highest | Steadiest levels, usually subcutaneous, most injections |
So is TRT better twice a week or once a week? For many men, twice weekly is the practical sweet spot: it roughly halves the peak-to-trough swing of a weekly shot without the daily commitment of a microdose 1. Some men who get side effects at the peak, or whose trough drops too far, do better on every-other-day or daily dosing. How often you inject TRT is a decision you make with your clinician based on your labs, your symptoms between doses, and how many injections you are willing to do. More frequent dosing is not automatically better for everyone; it is a tool for smoothing levels when that is the problem.
Microdosing TRT and Low-Dose Protocols
Microdosing TRT means splitting your weekly dose into small daily or every-other-day injections, usually given subcutaneously, to keep testosterone and estradiol as steady as possible 7. In practice a 100 to 160 mg weekly dose might be given as roughly 14 to 23 mg once daily, or about 25 to 40 mg every other day, rather than one or two larger shots. The rationale is a stable trough with a lower peak, which can mean fewer peak-related side effects (such as a sharp rise in red blood cell count or mood swings) and less estradiol conversion at the peak 7. Low dose TRT and daily TRT injections describe the same family of approaches.
The honest caveat is that head-to-head evidence that microdosing produces better long-term outcomes than twice-weekly dosing is still limited; much of the case for it is pharmacologic reasoning and clinical experience rather than large trials 7. It is a reasonable, physician-guided option for men who do not tolerate the peak of less frequent dosing, but it is not a mandatory upgrade, and the more frequent needles are a real trade-off. For where and how injections are given, see our guide to TRT injection sites.
Anastrozole and Estrogen Management on TRT
When testosterone rises, some of it converts to estradiol, and a common question is whether you need anastrozole (Arimidex) or another aromatase inhibitor to block that. For most men the answer is no. Both the Endocrine Society and the AUA guidelines do not recommend routine aromatase inhibitors as part of TRT, because moderate estradiol is normal and necessary in men, and over-suppressing it causes real harm 12. Estradiol that is too low in men is linked to joint pain, low libido, and, importantly, reduced bone mineral density, since estrogen (not just testosterone) is central to male bone health 9. Chasing a "low estrogen" number is one of the more common self-inflicted mistakes on TRT.
There is a narrow exception. If a man develops confirmed symptomatic gynecomastia with a genuinely elevated estradiol that does not resolve by lowering or splitting the testosterone dose, a clinician may use a low off-label dose of an aromatase inhibitor. Doses reported in clinics are small, on the order of 0.25 to 0.5 mg of anastrozole once or twice a week, and this is strictly physician-managed with follow-up estradiol testing 7. It is not a routine add-on, not a self-dosing protocol, and not a substitute for simply using the right testosterone dose. DIM and other over-the-counter "estrogen support" supplements do not have good evidence for this purpose. The first-line fix for high-estrogen symptoms is almost always to adjust the testosterone dose, not to add a blocker.
Signs Your TRT Dose Is Too High (and Too Low)
The clearest signs that your TRT dose is too high are lab and symptom changes that track with an excess of testosterone: a rising red blood cell count (hematocrit), new or worsening acne, fluid retention, elevated blood pressure, irritability or aggression, and disrupted sleep 710. The single most important of these is hematocrit, because a red blood cell count that climbs too high thickens the blood and raises clot risk, which is why it is monitored on every protocol 17. The correct response to dose-too-high symptoms is to lower the dose (or reduce the peak by splitting it), not to stack on additional drugs. There is no benefit to a "max TRT dosage" or a "highest TRT dose"; past the point that normalizes your levels, more testosterone adds side effects without adding replacement benefit.
The signs a dose is too low are the mirror image: your original low-testosterone symptoms (fatigue, low libido, low mood, poor recovery) persist because the trough level is still below target 1. The fix there is a measured increase or a frequency change, again guided by trough labs. For the fuller side-effect picture and how each is managed, see TRT side effects.
How Often to Give Blood on TRT
Testosterone stimulates red blood cell production, so a rising hematocrit is one of the most common reasons a dose is adjusted. Clinicians generally act when hematocrit reaches about 52 to 54% or higher, using a dose reduction, a switch of formulation, or therapeutic phlebotomy (a blood draw similar to donating) 7. How often you give blood on TRT is therefore not a fixed schedule; it is driven by your hematocrit readings, so some men never need it and others donate or have phlebotomy periodically. Injectable testosterone raises hematocrit more than transdermal gels do, which is one reason gels are sometimes preferred in men prone to a high red cell count 7. This is managed by your clinician from your labs, not self-directed.
Female TRT Dosage
Female TRT dosage is far smaller than male dosing, roughly one-tenth of a typical male dose, and transdermal delivery is preferred to avoid the supraphysiologic peaks that injections can cause 8. The Global Consensus Position Statement supports considering low-dose testosterone for postmenopausal women specifically for hypoactive sexual desire disorder, with blood levels kept within the normal premenopausal female range, and it does not endorse using testosterone in women for energy, mood, or general well-being on current evidence 8. There is no FDA-approved testosterone product for women in the US, so any use is off-label and prescriber-managed, and we do not publish a female milligram protocol here because the amount and monitoring belong with a clinician who can measure levels. For the full picture, see TRT for women.
TRT vs Tren, Nandrolone, and Anabolic "Stacks"
Searches like "tren vs trt," "nandrolone with trt," and "anavar trt cycle" conflate two very different things. Trenbolone, nandrolone, and oxandrolone (Anavar) are anabolic-androgenic steroids used to push muscle and performance above normal physiology; they are not testosterone replacement 11. TRT restores a low testosterone level back into the normal range and is dosed and monitored to stay there. Adding trenbolone or nandrolone to testosterone, or running an "anavar cycle," is supraphysiologic anabolic use that carries real cardiovascular, liver, cholesterol, and fertility risks that properly dosed replacement does not, and it is not TRT 11. This page gives no anabolic cycle instructions and no dosing for those compounds, because that is drug abuse, not replacement. For the clean distinction between replacement and steroid use, see is TRT a steroid.
Adjunct Medications: hCG, Gonadorelin, and Supplements
Some TRT protocols include adjunct medications, and it helps to separate the prescription ones from the supplements. hCG and gonadorelin are prescription drugs used, under a clinician, mainly to help preserve fertility and testicular volume during TRT, since external testosterone otherwise shuts down the body's own hormone signaling 12. They are physician-directed and dosed to the individual; if fertility matters to you, raise it before you start, and see TRT and fertility along with our guides to hCG and enclomiphene for how these options differ.
By contrast, pregnenolone, DHEA, and DIM are over-the-counter supplements frequently marketed as TRT companions, and the evidence for routinely adding them is weak to nonexistent 7. They are not required parts of a replacement protocol, and "pregnenolone dosage trt" or "dim trt" searches chase a benefit that is not established. Any adjunct is a conversation with your prescriber, not a self-assembled stack.
How Doctors Adjust Your TRT Dose
Dose setting on TRT is a monitored loop, not a one-time prescription. Before starting, clinicians confirm low testosterone on more than one morning blood test and check baseline labs 12. After a dose starts or changes, they typically recheck total and free testosterone (drawn at the trough, just before your next dose), along with hematocrit, estradiol, and PSA where age-appropriate, at about 6 to 8 weeks, then every 3 to 6 months until stable and roughly annually after that 123. Your clinician reads those numbers together with your symptoms to decide whether to hold, raise, lower, split, or switch your dose, which is why the same weekly milligram figure is right for one man and wrong for another. That lab-and-symptom loop, not a fixed chart, is what "best trt protocol" actually means in practice. For what the target numbers mean and how to read them, see our guide to testosterone levels on TRT.
Frequently Asked Questions
A normal TRT dose for injectable testosterone is about 100 to 200 mg of cypionate or enanthate per week, most often split into two or more injections and titrated to your labs 12. The goal is a mid-normal trough testosterone that resolves symptoms, not the top of the reference range, so the "normal" dose is really the one your blood work and symptoms land on.
Most men inject TRT once or twice a week, with twice weekly being the most common split because it steadies levels compared with a single weekly shot 1. Some protocols use every-other-day or daily microdosing for even steadier levels. How often you inject is set with your clinician based on your labs and how you feel between doses.
Twice a week is often the practical sweet spot: it roughly halves the peak-to-trough swing of a once-weekly injection without the effort of daily dosing 1. Once weekly is simpler but produces bigger hormone fluctuations. Neither is universally better; the right frequency is the one that keeps your trough on target and your side effects low.
Signs a TRT dose is too high include a rising red blood cell count (hematocrit), acne, fluid retention, higher blood pressure, irritability, and disrupted sleep 710. The fix is to lower or split the dose, not to add other drugs. Hematocrit is the key monitored marker, which is why bloodwork is part of every protocol.
200 mg per week is at the upper edge of the usual replacement range, not automatically too much, but as a single weekly shot it can push your peak level above normal 13. Whether it is appropriate depends on your trough labs and symptoms; many men are well replaced on less, so it is a decision for your prescriber, not a default target.
There is no fixed schedule; giving blood or having therapeutic phlebotomy on TRT is driven by your hematocrit, with clinicians typically acting when it reaches about 52 to 54% or higher 7. Some men never need it, while others donate periodically. Injectable testosterone raises hematocrit more than gels, so your monitoring and any phlebotomy are guided by your labs.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432.
- U.S. Food and Drug Administration. Depo-Testosterone (testosterone cypionate injection) Prescribing Information. 2025.
- U.S. Food and Drug Administration. AndroGel 1.62% (testosterone gel) Prescribing Information. 2016.
- U.S. Food and Drug Administration. Jatenzo (testosterone undecanoate oral capsules) Prescribing Information. 2018.
- U.S. Food and Drug Administration. FDA issues class-wide labeling changes for testosterone products. February 2025.
- Basheer B, et al. Management of Adverse Effects in Testosterone Replacement Therapy. Int Braz J Urol. 2025;51(3):e20259904.
- Davis SR, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J Clin Endocrinol Metab. 2019;104(10):4660-4666.
- Leder BZ, et al. Gonadal steroid-dependent effects on bone turnover and bone mineral density in men. J Clin Invest. 2016.
- Mayo Clinic. Testosterone therapy: Potential benefits and risks as you age. Accessed 2026.
- Cleveland Clinic. Testosterone Replacement Therapy (TRT). Accessed 2026.
- Drugs.com. Testosterone Dosage Guide + Max Dose, Adjustments. Accessed 2026.
- MedlinePlus. Testosterone Injection. U.S. National Library of Medicine. Accessed 2026.
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.