The main TRT injection sites are the gluteal muscle (buttock), the vastus lateralis (outer thigh), and the deltoid (shoulder) for intramuscular shots, plus the abdomen for subcutaneous injections. Here is the detail most guides skip: which of these sites you can actually use is not a free choice, it is set by the formulation your clinician prescribed. The FDA label for testosterone cypionate specifies deep intramuscular injection into the gluteal muscle 3, Xyosted is approved for subcutaneous injection in the abdomen only 4, and Aveed must be given as a deep gluteal injection in a healthcare setting 5. This guide walks through each site, intramuscular versus subcutaneous, needle sizes, technique, and rotation, so you know exactly what to expect and what to ask your prescriber.
Key Takeaways
- Four sites cover almost all TRT injections: the gluteal muscles, the outer thigh (vastus lateralis), and the deltoid for intramuscular shots, and the abdomen for subcutaneous shots 679.
- Your formulation decides your site. Testosterone cypionate is labeled for deep gluteal intramuscular injection 3, Xyosted for subcutaneous abdominal injection only 4, and Aveed for in-office deep gluteal injection only 5.
- Subcutaneous and intramuscular both work. In a 2021 study of 234 men, subcutaneous testosterone enanthate produced testosterone levels comparable to intramuscular cypionate, with lower hematocrit and estradiol at 12 weeks 8.
- Needle size depends on route: most intramuscular injections use a 22 to 25 gauge needle 1 to 1.5 inches long, while subcutaneous injections use a shorter, thinner 25 to 30 gauge needle around half an inch 69.
- Rotate your sites. Repeated injections in one spot raise the odds of scar tissue, soreness, and inconsistent absorption, so most clinicians recommend a simple rotation schedule 69.
- Get trained before you self-inject. Testosterone is a Schedule III prescription medicine, and guidelines and labels expect your first doses to be supervised by a clinician 36.
TRT injection site quick reference:
| Site | Route | Typical needle | Best for | Notes |
|---|---|---|---|---|
| Gluteal (ventrogluteal or dorsogluteal) | Intramuscular | 22-25G, 1-1.5 in | Cypionate per its FDA label; larger volumes | Ventrogluteal is the safest IM landmark; dorsogluteal sits nearer the sciatic nerve 39 |
| Vastus lateralis (outer thigh) | Intramuscular | 22-25G, 1-1.5 in | Self-injection at home | Easiest site to see and reach on yourself 69 |
| Deltoid (shoulder) | Intramuscular | 22-25G, 1 in | Small injection volumes | Smaller muscle; not ideal for larger oil volumes 9 |
| Abdomen | Subcutaneous | 25-30G, about 0.5 in | Xyosted per its FDA label; low-pain routine | Inject into pinched skin fold, 2 inches away from the navel 4 |
What Is a TRT Injection?
A TRT injection (often called a TRT shot) is a dose of prescription testosterone delivered into muscle or into the fat under the skin as part of testosterone replacement therapy for diagnosed hypogonadism, meaning the body does not make enough of its own testosterone 1011. Injectable TRT is the most commonly prescribed form because it is effective, inexpensive, and dosed on a predictable schedule 110.
Two things set injectable testosterone apart. It is a Schedule III controlled substance, available only by prescription for a diagnosed medical need 3, and the common forms (testosterone cypionate and enanthate) are dissolved in oil that absorbs slowly, which is why a single injection can cover a week or more 34. Both the Endocrine Society and the American Urological Association recommend confirming low testosterone with at least two morning blood tests plus symptoms before starting any injections 12.
TRT Injection Sites: Your Main Options
There are four standard TRT injection sites, and each maps to a route and, in practice, to a formulation:
- Gluteal muscle (buttock). The classic deep intramuscular site. The Depo-Testosterone (testosterone cypionate) label directs injection deep into the gluteal muscle 3, and Aveed (testosterone undecanoate) is also given as a deep gluteal injection, but only by a healthcare provider in a clinic 5.
- Vastus lateralis (outer thigh). A large, easy-to-reach muscle that clinicians commonly teach for at-home intramuscular self-injection 69.
- Deltoid (shoulder). A smaller intramuscular option suited to smaller injection volumes 9.
- Abdomen (subcutaneous). The only FDA-labeled site for Xyosted, the weekly testosterone enanthate autoinjector, which is injected into the fat of the abdomen 4. Many clinicians also prescribe off-label subcutaneous injections of cypionate drawn from a vial.
The practical takeaway: do not pick a site off a chart and improvise. Ask your prescriber which route your medicine is approved for and where they want you to inject. The formulation itself is a shared decision based on pharmacokinetics, convenience, cost, and your preference 1.
TRT Intramuscular vs Subcutaneous
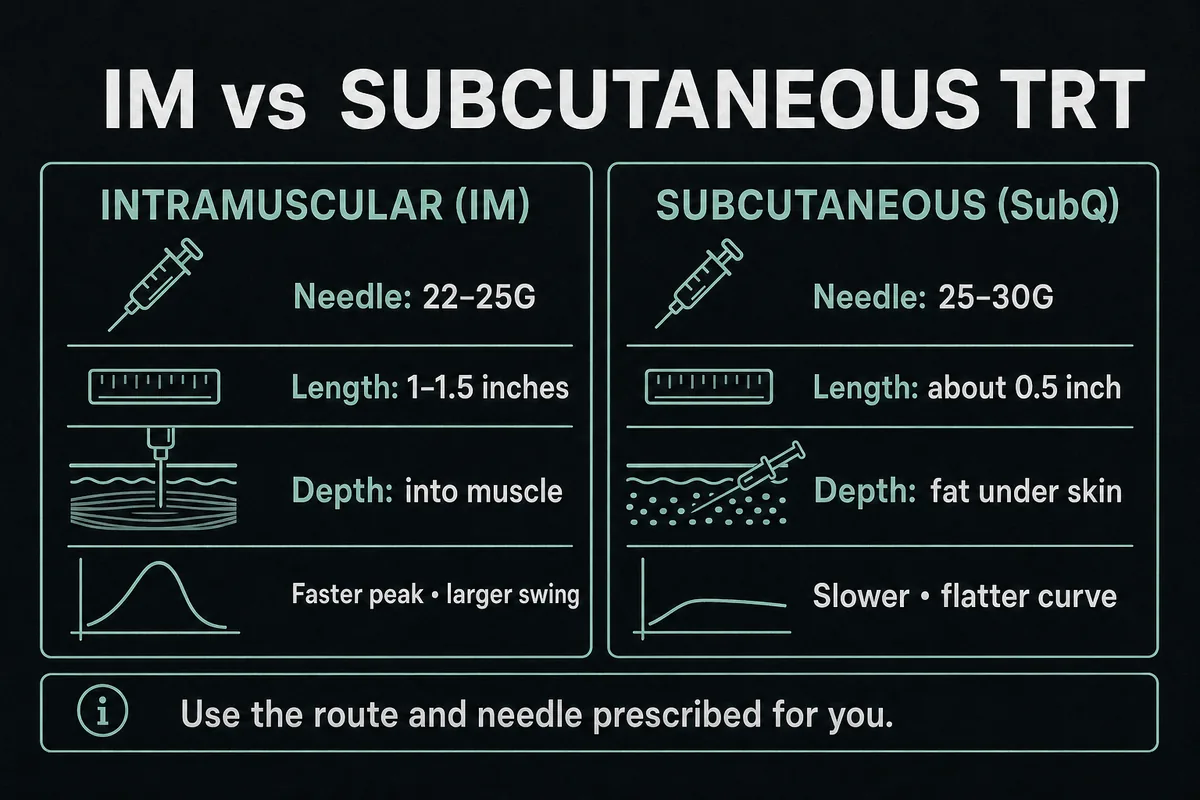
The TRT subq vs IM question comes down to depth. Intramuscular (IM) injections deposit the oil deep in a muscle, which has a rich blood supply and absorbs the dose over days. Subcutaneous (subQ) injections place it in the fat layer under the skin, where absorption is somewhat slower and steadier. Mayo Clinic lists both routes as accepted ways to give testosterone, depending on the product 7.
| Factor | Intramuscular (IM) | Subcutaneous (SubQ) |
|---|---|---|
| Needle | 22-25G, 1-1.5 inches | 25-30G, about 0.5 inches |
| Depth | Deep into muscle | Fat layer under the skin |
| Absorption | Faster peak, larger peak-to-trough swing | Slower, flatter curve |
| Typical formulations | Testosterone cypionate, enanthate from a vial; Aveed (in office) 35 | Xyosted autoinjector; off-label cypionate/enanthate 4 |
| Hematocrit and estradiol signal | Higher in one 12-week comparison 8 | Lower hematocrit and estradiol in the same study 8 |
| Self-injection ease | Longer needle, more technique to learn | Shorter needle, generally easier and less intimidating |
What the research says about subcutaneous TRT
The best direct comparison to date is a 2021 study in the Journal of Urology that followed 234 hypogonadal men on either intramuscular testosterone cypionate or subcutaneous testosterone enanthate. At 12 weeks, both groups reached comparable testosterone levels, while the subcutaneous group showed lower hematocrit (the red blood cell measure TRT can push up) and lower estradiol 8. That does not prove subQ is better for everyone; it means subcutaneous dosing is a legitimate, evidence-supported option to discuss with your clinician, especially if hematocrit creeps up on IM dosing. Your lab monitoring, covered in our guide to testosterone levels on TRT, stays the same either way.
TRT Glute Injection Site
The glute is the traditional answer to where to inject TRT, and it is the site named on the cypionate and Aveed labels 35. It is a large muscle that comfortably handles a 1 mL oil injection, and injecting the upper outer area keeps the needle away from major nerves when done correctly.
The trade-off is access. Reaching your own upper outer buttock at the right angle is awkward, which is why many glute injectors have a partner help, or switch to the thigh for self-injection 6.
Ventrogluteal vs dorsogluteal
There are actually two gluteal sites. The dorsogluteal site is the old-school upper outer quadrant of the buttock; the ventrogluteal site is on the side of the hip, over the gluteus medius. Current injection-technique guidance in StatPearls identifies the ventrogluteal site as the safest intramuscular option, with a thinner fat layer over the muscle and distance from the sciatic nerve and superior gluteal vessels 9. The same reference notes that aspiration (pulling back the plunger to check for blood) is now reserved for dorsogluteal injections rather than required everywhere 9. If you inject in the glute, ask your clinician to mark the ventrogluteal landmark for you; how to inject TRT in the glute safely is mostly a matter of learning that spot once, hands-on.
TRT Thigh Injection Site
For self-injectors, the thigh is usually the most practical intramuscular site. The target is the vastus lateralis, the muscle on the outer front of the thigh. To find where to inject TRT in the thigh, sit down, divide the distance between the top of your thigh and your knee into thirds, and use the outer middle third 69. You can see the site, reach it with both hands, and control the needle angle, which makes technique errors less likely than twisting around to reach your glute.
People sometimes call this the TRT quad injection site, which is close enough anatomically since the vastus lateralis is one of the four quadriceps muscles. Keep the injection on the outer portion of the thigh, not the top or inner side, to stay in the right muscle and away from larger vessels and nerves 9. Some people notice more soreness in the thigh than the glute in the first weeks; slower injection and proper depth usually help.
TRT Deltoid (Shoulder) Injection
The deltoid is the muscle you know from vaccines, and it works as a TRT shoulder injection site with one caveat: it is small. Injection-technique references recommend keeping deltoid volumes small, which suits lower-volume TRT doses, particularly when a weekly protocol splits the dose into smaller shots 9. The landmark is roughly 2 to 3 finger widths below the acromion, the bony point at the top of the shoulder, injecting into the thickest part of the muscle.
The deltoid is convenient because it needs no undressing and is easy to alternate left and right. It is a poor choice for larger oil volumes, which belong in the glute or thigh, and repeated shots into a small muscle make rotation more important, not less 9.
Subcutaneous TRT Injection Sites
Subcutaneous TRT injection sites are the abdomen and, in some off-label protocols, the fatty area of the upper outer thigh. The abdomen is the only site in the Xyosted label: the autoinjector is pressed into a pinched fold of belly fat at least 2 inches away from the navel, alternating sides each week 4.
If your clinician prescribes subcutaneous injections drawn from a regular cypionate or enanthate vial (a common off-label approach), the technique is the pinch method: clean the skin, pinch a fold of fat, insert the short needle into the fold at the angle your clinician taught you, and inject slowly 6. The needle is small enough that most people find subQ shots nearly painless, a real adherence advantage over a weekly 1.5 inch intramuscular needle. Because this route is off-label for vial products, confirm it with your prescriber rather than a forum.
Best TRT Injection Site: How to Choose
There is no single best TRT injection site for everyone, and the decision runs in a specific order:
- Formulation first. Xyosted means the abdomen, full stop 4; Aveed means the glute, at the clinic 5. Cypionate's label points to the gluteal muscle for deep IM injection 3, with thigh and deltoid used in practice under clinician direction, and subQ used off-label when your prescriber recommends it.
- Self-injection ease second. If you inject yourself, the outer thigh (IM) or abdomen (subQ) are the sites you can see and reach reliably.
- Comfort and tolerance third. Within your prescriber's approved options, it is fine to prefer the site that hurts least.
- Rotation capacity last. Whichever site you favor, you need at least a left/right pair to alternate.
The Endocrine Society frames formulation choice itself as a shared decision built on pharmacokinetics, treatment burden, cost, and patient preference 1, and site choice inherits that logic. If you are still weighing injections against gels or pellets in the first place, start with our overview of the types of TRT.
TRT Needle Size: Gauge and Length
TRT needle size trips people up because you ideally use two needles per injection: a wider one to draw the thick oil out of the vial, and a fresh, finer one to inject. Swapping to a new needle after drawing also means you inject with a sharp tip, which hurts less.
| Purpose | Gauge | Length |
|---|---|---|
| Drawing from the vial | 18-20G | 1-1.5 in |
| Intramuscular injection | 22-25G | 1-1.5 in (glute/thigh); 1 in often fits the deltoid |
| Subcutaneous injection | 25-30G | About 0.5 in |
Higher gauge means a thinner needle. For intramuscular injections, length matters as much as gauge: the needle has to pass through the fat layer and reach muscle, which is why 1 to 1.5 inches is standard for the glute and thigh in adults 9. For subcutaneous injections, many clinicians have patients use insulin-style syringes in the 27 to 30 gauge range with a half-inch needle. What size needle for a TRT injection ultimately depends on your route, body composition, and dose volume, so treat your prescriber's instructions as the final word 6.
How to Inject TRT: Step by Step
This is an educational outline of how to inject TRT, not a substitute for in-person training. MedlinePlus advises that a doctor or nurse gives the first injection and teaches you the technique before you ever inject alone 6.
- Wash your hands and gather supplies: vial, draw needle, injection needle, syringe, alcohol swabs, gauze, and a sharps container 6.
- Inspect the solution. Testosterone injection should be clear to light yellow with no particles floating in it; do not use it otherwise 6.
- Draw the dose with the 18-20G needle, then switch to your fresh injection needle and expel air.
- Clean the site with an alcohol swab and let it dry.
- Inject with the right technique for your route. For IM, insert at 90 degrees into the muscle; the Z-track method (pulling the skin sideways before inserting, then releasing after) reduces leak-back and irritation 9. Aspiration is reserved for dorsogluteal injections 9. For subQ, pinch a fold of fat and inject into the fold 46.
- Inject slowly, withdraw, and apply gentle pressure. Do not rub the site hard.
- Dispose of needles in a sharps container, never household trash 6.
If a step ever feels uncertain, stop and call your clinic rather than improvising. And if you are early in treatment and wondering when injections start paying off, see how long TRT takes to work.
TRT Injection Site Rotation
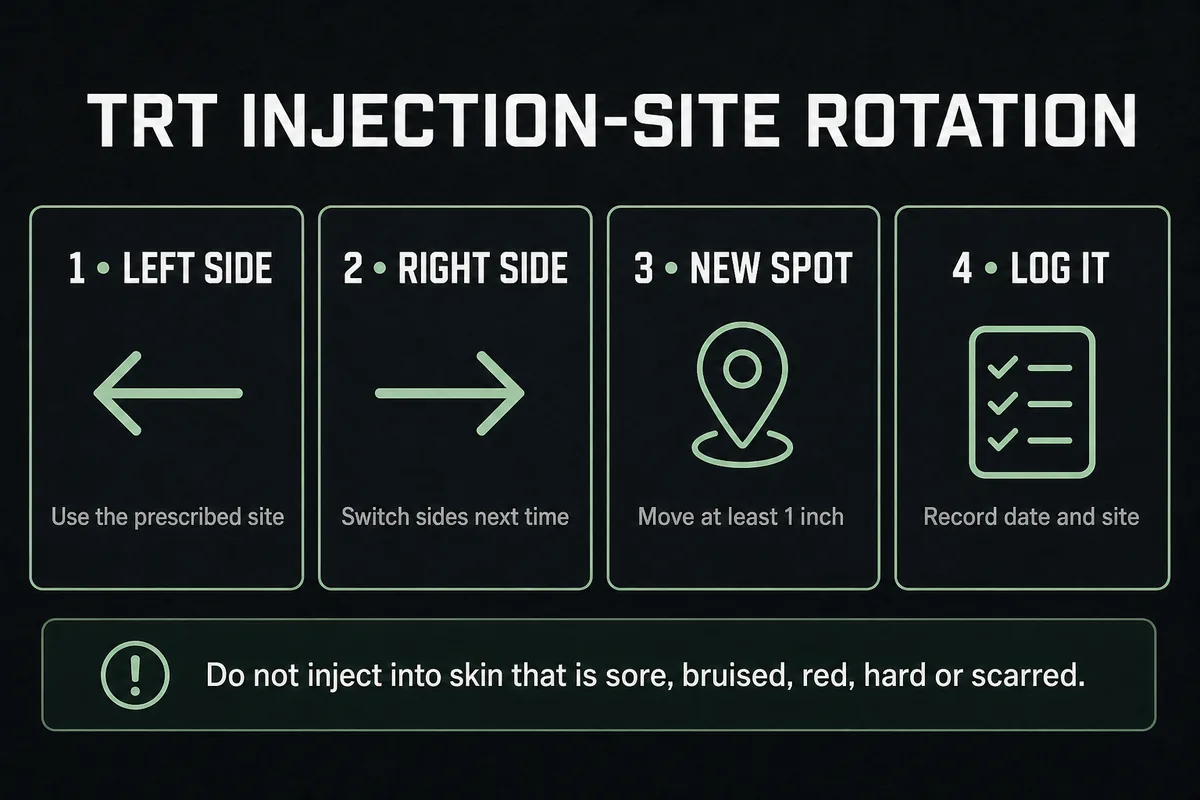
TRT injection site rotation means never injecting the same exact spot twice in a row. Repeated injections into one location can build scar tissue and lumpy, fibrous areas, cause more soreness, and make absorption less predictable 69.
Rotation can be simple:
- 2-site rotation: left thigh, right thigh, alternating each injection. The minimum viable plan for weekly shots.
- 4-site rotation: left thigh, right thigh, left glute, right glute. A full month between repeat visits on weekly dosing.
- 6-site rotation: add left and right deltoid for smaller volumes, or left and right abdomen for subQ users.
Keep a simple log so you always know which site is next. If a previous site is still sore, hard, or discolored when its turn comes around, skip it and mention it at your next appointment.
TRT Injection Schedule and Best Time of Day
Your TRT injection schedule comes from your prescriber and your formulation. The cypionate label allows 50 to 400 mg every two to four weeks 3, but in modern practice many clinicians prescribe smaller doses weekly or twice weekly to smooth out peaks and troughs, and Cleveland Clinic describes weekly self-injection as typical 10. Xyosted is a fixed weekly subcutaneous injection 4, and Aveed follows a long-interval in-office schedule 5. Dose and interval interact, which is covered in detail in our TRT dosage guide.
As for the best time of day for a TRT injection: with oil-based esters that release over days, the clock time of your shot has no meaningful effect on results, so consistency matters more than timing. Pick a day (and a time you will remember), keep it stable, and your levels settle into a repeatable weekly pattern. What does matter is when you draw labs relative to your injection, since levels peak and then fall between doses 3; your clinician will usually standardize lab timing so results are comparable.
Managing Pain, Lumps, and Other Side Effects
Some post-injection effects are common and mild; a few deserve a call to your clinician. For the systemic side of treatment (hematocrit, estradiol, fertility, and more), see our full guide to TRT side effects. At the injection site specifically:
- TRT injection site pain (PIP). Soreness for a day or two after an intramuscular oil injection is common, especially early on. Slower injection, room-temperature oil, an appropriate needle length, and rotating sites all help. Pain that worsens after 48 hours, spreads, or comes with fever is a reason to call your clinician 6.
- A lump or hard knot. A small, firm TRT injection site lump usually reflects a pocket of oil still absorbing or local irritation, and it typically resolves over days. A lump that keeps growing, gets red and hot, or drains is potentially an infection or abscess and needs medical review 6.
- A little blood after injecting. Nicking a small surface vessel on the way in is harmless; press gauze on it. Recurrent significant bleeding or a large bruise is worth mentioning at your next visit.
- Coughing right after the shot. A sudden cough or urge to cough during or right after an oil injection can be pulmonary oil microembolism (POME), tiny oil droplets reaching the lungs. It is formally described in the Aveed boxed warning, which is why that product is injected in-office with a 30 minute observation period 5. Brief episodes usually resolve on their own, but chest pain, trouble breathing, dizziness, or fainting after any injection warrants urgent care 56.
TRT Injections vs Creams, Gels, and Pellets
Injections are not the only option. Daily gels and creams keep levels steady but carry a skin-transfer risk to partners and children 710. Implanted pellets last months but require a minor office procedure and cannot be adjusted once placed 10. Oral testosterone undecanoate capsules are dosed twice daily with food and cost more 10. Injections win on cost, dosing control, and infrequent administration, at the price of needles and a peak-trough pattern 110. The full comparison lives in our guide to the types of TRT; the Endocrine Society treats this as a preference-and-logistics decision between you and your clinician, not a ranking 1.
Can You Do TRT Injections at Home?
Yes. At-home TRT injections are standard practice once two conditions are met: you have a legitimate prescription from a licensed clinician after proper diagnosis, and you have been trained in person on your specific route and site 610. MedlinePlus is explicit that the first dose should be given in a medical setting and that self-injection starts only after your prescriber confirms you can do it correctly 6. From there, most people on cypionate or Xyosted manage their own weekly shots at home with periodic lab monitoring per AUA and Endocrine Society guidance 12.
Two cautions. Testosterone is a Schedule III controlled substance; buying it without a prescription is illegal and skips the diagnosis, dosing, and monitoring that make TRT safe 311. And "at home" does not mean "on your own": lab work, dose changes, and site or route changes should all run through your prescribing clinician.
Frequently Asked Questions
TRT is injected either into a muscle (the gluteal muscle, outer thigh, or deltoid) or into the fat under the skin of the abdomen, depending on the product 67. Your prescribed formulation narrows the choice: cypionate's label specifies the gluteal muscle, while Xyosted is abdomen-only subcutaneous 34.
Most intramuscular TRT injections use a 22 to 25 gauge needle, 1 to 1.5 inches long, while subcutaneous injections use a 25 to 30 gauge needle around half an inch long 9. Draw the oil with a wider 18-20G needle, then switch to a fresh needle to inject.
With oil-based injectable testosterone, the time of day does not meaningfully change your results, because each dose releases over days 3. Pick a consistent day and time you will not miss, and keep lab draws consistently timed relative to your injection.
A sudden cough right after an oil-based injection can be pulmonary oil microembolism (POME), where tiny oil droplets reach the lungs; it is documented in the boxed warning for Aveed 5. Brief coughing usually passes, but chest pain, trouble breathing, or feeling faint after an injection should be treated as urgent 56.
A small firm lump is usually a depot of oil that has not fully absorbed yet, or mild local irritation, and it generally resolves within days 6. If a lump grows, becomes red, warm, or painful, or you develop a fever, contact your clinician to rule out infection.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, 2018.
- American Urological Association. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol, 2018.
- Depo-Testosterone (testosterone cypionate) FDA prescribing information. DailyMed, National Library of Medicine.
- Xyosted (testosterone enanthate) FDA prescribing information. DailyMed, National Library of Medicine.
- Aveed (testosterone undecanoate) FDA prescribing information. DailyMed, National Library of Medicine.
- Testosterone Injection. MedlinePlus, National Library of Medicine.
- Testosterone (Intramuscular Route, Subcutaneous Route). Mayo Clinic.
- Pastuszak AW, et al. Comparison of Outcomes for Hypogonadal Men Treated with Intramuscular Testosterone Cypionate versus Subcutaneous Testosterone Enanthate. J Urol, 2021.
- Polania Gutierrez JJ, Munakomi S. Intramuscular Injection. StatPearls, NCBI Bookshelf.
- Cleveland Clinic. Testosterone Replacement Therapy (TRT).
- Cleveland Clinic. Low Testosterone (Male Hypogonadism).
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.