
Testosterone levels on TRT are not about chasing the highest possible number, they are about landing in the mid-normal range that resolves your symptoms safely. In practice the American Urological Association (AUA) describes a treatment target of roughly 450 to 600 ng/dL (about 15.6 to 20.8 nmol/L), while the Endocrine Society aims for the mid-normal range, roughly 400 to 700 ng/dL (about 13.9 to 24.3 nmol/L), measured around a week after a weekly injection 12. Before any of those numbers matter for you, one thing has to be clear: testosterone is a prescription, Schedule III controlled therapy, every range here is educational, and your own target and dose are set by your prescriber from your labs and your symptoms, not from an article. If you are new to the topic, start with our pillar guide to testosterone replacement therapy, then use this page to read your bloodwork.
Key Takeaways
- The target is mid-normal, not maximal. The AUA describes treating to roughly 450 to 600 ng/dL and the Endocrine Society aims for the mid-normal range (about 400 to 700 ng/dL measured a week after a weekly injection), not the top of the reference range 12.
- Free testosterone matters as much as total. Only about 1 to 3 percent of your testosterone is free and biologically active, so the free fraction, not just the total, drives how you feel 6.
- Timing of the draw changes the number. A peak reading and a trough reading can differ substantially, so pick one consistent point and stick with it every time 18.
- A full panel is required, not just total T. Total and free testosterone, estradiol, hematocrit, and PSA all belong on a TRT blood test, because the safety of therapy lives in those extra numbers 14.
- You should never run TRT without bloodwork. Diagnosis needs two morning draws below 300 ng/dL, and ongoing hematocrit and PSA monitoring is a safety requirement, not optional 124.
- Higher-than-normal levels are not the guideline target. The supraphysiologic numbers some influencers cite raise hematocrit and other risks and are an optimization choice, not the replacement target the evidence supports 111.
| Metric | Value |
|---|---|
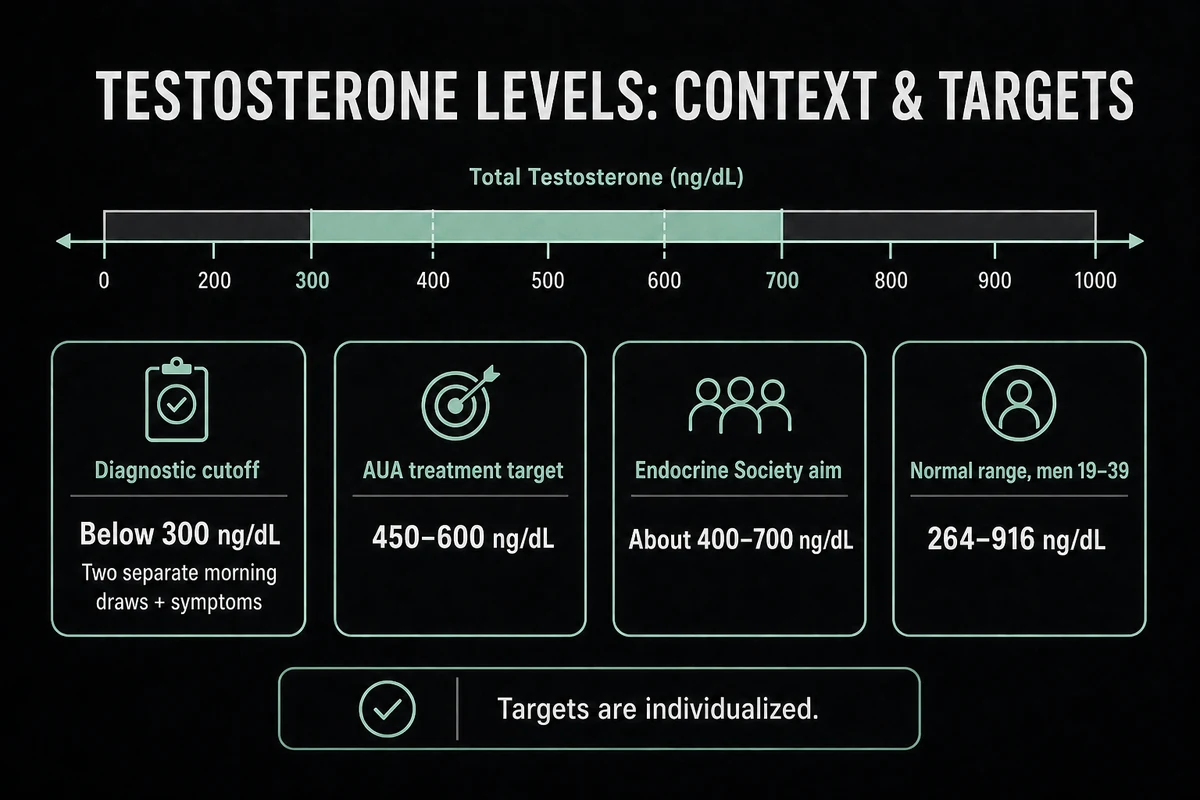
| Diagnostic cutoff for TRT | Total testosterone below 300 ng/dL (about 10.4 nmol/L) on two separate morning draws 27 |
| AUA treatment target | Roughly 450 to 600 ng/dL (about 15.6 to 20.8 nmol/L) 2 |
| Endocrine Society aim | About 400 to 700 ng/dL (about 13.9 to 24.3 nmol/L), roughly one week after a weekly injection 1 |
| Normal reference range (men 19 to 39) | 264 to 916 ng/dL (about 9.2 to 31.8 nmol/L), median 531 3 |
| Free testosterone | About 1 to 3 percent of total testosterone, the active fraction 6 |
| Hematocrit action threshold | Above 54 percent means hold or reduce therapy 14 |
| First follow-up labs | Around 3 to 6 months after starting, then annually once stable 14 |
What Are Ideal Testosterone Levels on TRT?
The question behind "ideal testosterone levels on trt," "test levels for trt," and "testosterone levels for trt" has a cleaner answer than the internet suggests: the ideal level is the one inside the normal range that relieves your symptoms at the lowest effective dose. The AUA frames the treatment target as the normal physiologic range of about 450 to 600 ng/dL (about 15.6 to 20.8 nmol/L), reached with the minimum effective dose 2. The Endocrine Society describes aiming for the mid-normal range, and for weekly testosterone cypionate or enanthate it references a level of roughly 400 to 700 ng/dL (about 13.9 to 24.3 nmol/L) measured about a week after the injection 1.
To put that in context, the harmonized normal reference range for healthy nonobese men aged 19 to 39 is 264 to 916 ng/dL (about 9.2 to 31.8 nmol/L), with a median of 531 ng/dL (about 18.4 nmol/L) 3. Notice that the treatment target sits in the middle of that band, not at the ceiling. That is deliberate. The goal of replacement is to restore a normal level, and both the FDA labeling and the guidelines describe titrating into the normal range rather than pushing above it 14. Where you land inside the window is individual: two men at the same 550 ng/dL can feel different, which is why the number supports the decision but symptoms lead it.
A quick note on units. US labs report testosterone in ng/dL, and the rest of the world usually reports nmol/L. To convert, multiply ng/dL by 0.0347. This page gives ng/dL first with the nmol/L conversion in parentheses so the numbers work wherever you are. How a specific weekly dose maps onto a given blood level is covered in our guide to TRT dosage.
What Testosterone Level Qualifies for TRT?
For "what testosterone level for trt," "testosterone level for trt," and "test levels for trt," the diagnostic bar is stricter than many expect. A diagnosis of hypogonadism generally requires a total testosterone below 300 ng/dL (about 10.4 nmol/L), confirmed on two separate early-morning blood draws, together with symptoms of low testosterone 27. One low reading is not enough, because testosterone swings through the day and dips with illness, poor sleep, or acute stress, so the morning timing and the repeat test both matter 8.
The other half of the definition is symptoms. A number below 300 ng/dL without any symptoms is not automatically treated, and normal age-related decline is not, by itself, a reason to start testosterone. Both the FDA and Mayo Clinic are explicit that testosterone products are approved for men with a medically diagnosed cause of hypogonadism, not for the normal dip that comes with aging 59. In 2025 the FDA reinforced this in class-wide labeling changes, keeping the indication to diagnosed hypogonadism and adding a blood-pressure warning 5. TRT is treatment for a confirmed deficiency, not a lifestyle upgrade.
Total vs Free Testosterone: Which Number Matters on TRT
When people search "free testosterone levels on trt" or "trt free testosterone levels," they have usually realized that the total number does not tell the whole story. Your total testosterone is the sum of two parts: the fraction bound to proteins (mainly sex hormone binding globulin, or SHBG, and albumin) and the small free, unbound fraction. Only about 1 to 3 percent of your testosterone circulates free, and that free portion, along with the loosely albumin-bound share, is what is actually available to your tissues 6. That is why a man with a "normal" total but high SHBG can still feel deficient: too much of his testosterone is locked up.
So, does TRT increase free testosterone? Yes. Adding exogenous testosterone raises both total and free testosterone, and because higher testosterone can modestly lower SHBG, the free fraction often rises a little more than the total alone would suggest 6. That is also why clinicians look at both numbers: two men can share a total of 600 ng/dL while their free testosterone diverges because their SHBG differs.
Free testosterone reference ranges are assay-dependent, which is the important caveat. Commonly reported adult male free testosterone ranges run in the neighborhood of 5 to 21 ng/dL (roughly 50 to 210 pg/mL), but the exact numbers vary by laboratory and method, and there is no single universally agreed "ideal free T on TRT" figure. The most reliable measurements come from equilibrium dialysis or a calculated free testosterone (using total T, SHBG, and albumin) rather than older direct immunoassays 68. The practical target most clinicians use is to keep total testosterone mid-normal while free testosterone sits in the upper part of that lab's reference range, judged alongside symptoms. If you are weighing supplements against actual therapy, our comparison of testosterone boosters versus peptides explains why over-the-counter "free T boosters" do not move these numbers the way prescription therapy does.
How to Increase Free Testosterone on TRT
The honest answer to "how to increase free testosterone on trt" is that the levers belong to your prescriber, not to a supplement aisle. The real, physician-managed options are: adjusting the dose or injection frequency so your trough does not fall too low; addressing factors that raise SHBG (which include some medications and thyroid status); and choosing a formulation and schedule that keep levels steady. Weight loss and better sleep can modestly lower SHBG and lift the free fraction over time 910. What does not work, and what clinicians actively warn against, is chasing free testosterone by pushing the dose above the normal range: that inflates hematocrit and other risks without a proportional benefit, and it moves you out of the replacement target into supraphysiologic territory 111. This is a lab-guided adjustment made with your clinician, never a do-it-yourself protocol.
Free and Total Testosterone Target Table (ng/dL and nmol/L)
The table below pulls the total and free testosterone numbers together in dual units. It owns the practical intent behind "test levels for trt," "trt test levels," and "what testosterone level for trt": what qualifies you, what clinicians treat toward, and how the reference range differs from the target. Remember the conversion, ng/dL multiplied by 0.0347 gives nmol/L.
| Marker | Low end | Typical TRT target | Units note |
|---|---|---|---|
| Total testosterone (diagnostic) | Below 300 ng/dL (below ~10.4 nmol/L) qualifies with symptoms | n/a | Two separate morning draws confirm the diagnosis 27 |
| Total testosterone (on treatment) | Around 450 ng/dL (~15.6 nmol/L) | About 450 to 700 ng/dL (~15.6 to 24.3 nmol/L), mid-normal | AUA ~450 to 600; Endocrine Society aims mid-normal, ~400 to 700 one week post-injection 12 |
| Free testosterone | Assay-dependent, often around 5 ng/dL (~50 pg/mL) | Upper part of the lab's normal reference range | About 1 to 3 percent of total; equilibrium dialysis or calculated is most reliable 6 |
| Normal reference range (19 to 39) | 264 ng/dL (~9.2 nmol/L) | Context only, not a target | Median 531 ng/dL (~18.4 nmol/L) 3 |
These are ranges guidelines and labs describe, not a prescription. Your target and dose are set by your clinician from your own labs and symptoms.
TRT Blood Test: The Full Lab Panel
A proper TRT blood test is far more than a single total testosterone reading, and the searches for "trt labs," "trt lab," "trt bloodwork," "trt blood work," "blood work for trt," and "trt blood test panels" all point at the same need: knowing what belongs on the panel and why. The safety of therapy lives in the numbers beyond testosterone itself. The AndroGel label, representative of testosterone product labeling, directs clinicians to measure serum testosterone and titrate to the normal range, and to check hematocrit at 3 months, 6 months, and then annually, along with PSA and other markers 4. The Endocrine Society similarly ties monitoring to testosterone, hematocrit, and PSA on a schedule 1.
The table below is the panel most clinics run, with when each test is done and what it is telling your clinician. This is the safety net that turns a list of risks into managed ones. Two items on it link out for more depth: the hematocrit story is covered in TRT side effects, and how your formulation changes both your level and your draw timing is covered in types of TRT.
| Test | When to test | Why it matters |
|---|---|---|
| Total testosterone | Baseline, then 3 to 6 months, then annually | Confirms deficiency and tracks whether you are in the target range 12 |
| Free testosterone | Baseline and with symptoms that do not fit the total | Reflects the active fraction; useful when SHBG is high or low 6 |
| SHBG | Baseline and when free and total T disagree | Explains why free testosterone is high or low for a given total 6 |
| Sensitive estradiol (E2) | Baseline, then if symptoms suggest | Testosterone converts to estradiol; too high or too low both cause symptoms 1 |
| CBC / hematocrit | Baseline, 3 months, 6 months, then annually | Testosterone raises red blood cell count; above 54 percent means hold therapy 14 |
| PSA | Baseline, then per age and risk during treatment | Screens the prostate; a meaningful rise prompts urology review 4 |
| Lipid panel | Baseline and periodically | Tracks cholesterol changes on therapy 4 |
| Metabolic panel (CMP) | Baseline and periodically | Checks liver and kidney function and electrolytes 4 |
| LH and FSH | Baseline | Distinguishes primary from secondary hypogonadism 7 |
| Prolactin | Baseline | Screens for a pituitary cause of low testosterone 7 |
TRT Blood Test Timing: Peak, Trough, or Mid-Cycle
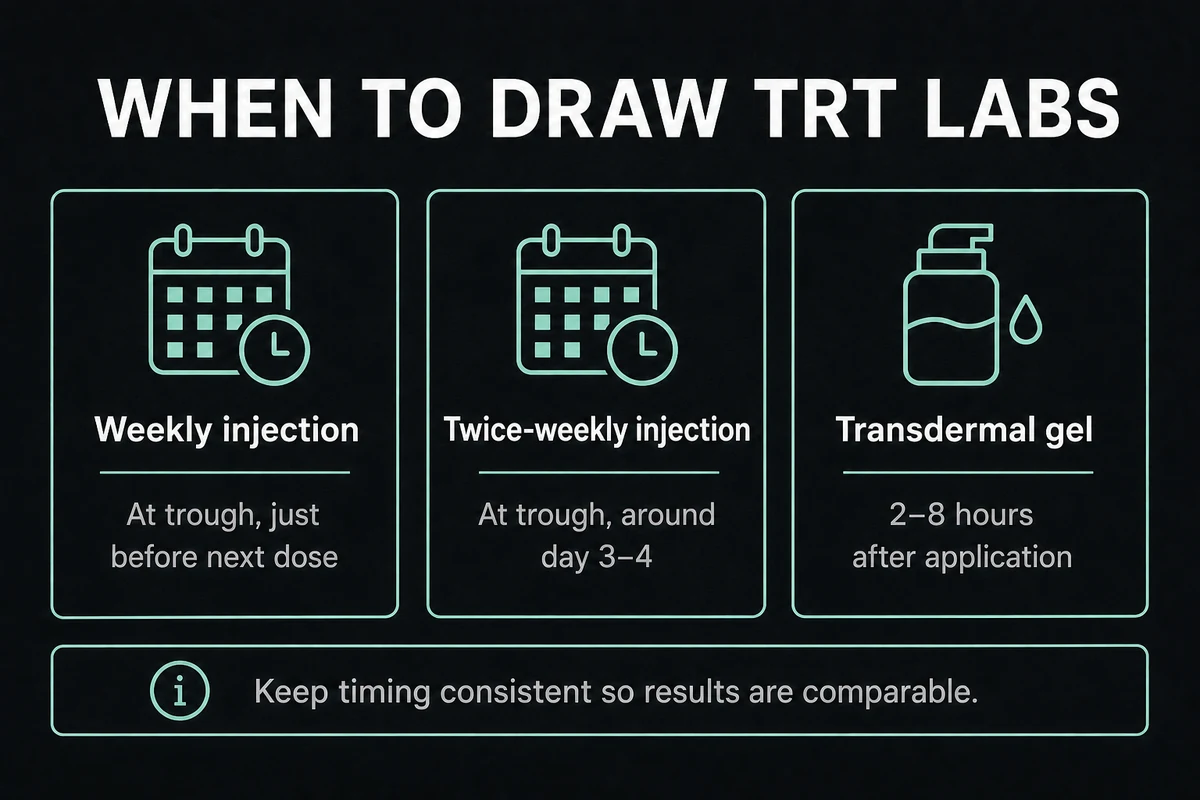
Competitors disagree on this, which is exactly why "trt blood test timing" is worth answering plainly. The single rule that matters more than any specific hour is consistency: draw at the same point in your cycle every time, or the numbers cannot be compared. Within that rule, the convention depends on your formulation. For a weekly injection, many clinics draw at trough (just before the next dose) to confirm the level is not dropping too low, while the Endocrine Society references a mid-interval reading of roughly 400 to 700 ng/dL about a week after a weekly shot 1. Gels are drawn a few hours after application once absorption has stabilized over a couple of weeks. Oral testosterone undecanoate has its own label-specified window tied to a meal.
| Formulation | When to draw | Why |
|---|---|---|
| Weekly IM or SC cypionate/enanthate | At trough (just before the next dose), or about 1 week post per Endocrine Society | Trough confirms the low point is adequate; the mid-interval reading maps to the guideline target 1 |
| Twice-weekly injection | At trough, around day 3 to 4 | Smaller swings; the trough is the meaningful low point 1 |
| Transdermal gel | About 2 to 8 hours after application, after roughly 2 weeks of use | Levels stabilize after steady daily use; draw once absorption is at steady state 4 |
| Oral testosterone undecanoate | Per the product label window, timed to a meal | Absorption is food-dependent, so the label window standardizes it 8 |
Whatever you and your clinician choose, keep the timing identical each time so your results are comparable.
When Does TRT Reach Steady Levels?
Levels do not stabilize the day you start. For injectable testosterone, blood levels generally reach a steady state over about 4 to 6 weeks, which is why the first follow-up labs are usually drawn a few months in rather than after the first shot 1. Symptom benefits lag the blood level and build over months, not days. That gap between "my level is in range" and "I feel the full benefit" is normal and expected, and our guide to how long TRT takes to work walks through the realistic timeline.
Can You Do TRT Without a Blood Test?
For "trt without blood test," the answer is a firm, guideline-backed no. Diagnosis itself requires bloodwork: two separate morning total testosterone measurements below 300 ng/dL (about 10.4 nmol/L) are needed to confirm hypogonadism before therapy is even appropriate 27. Skipping that step means treating a condition you have not confirmed you have.
Monitoring is not optional either. Testosterone raises your red blood cell count, and guidelines and product labeling direct clinicians to check hematocrit at baseline, at 3 and 6 months, and then annually, holding therapy if hematocrit climbs above 54 percent because of the clotting risk 14. PSA is tracked for the prostate, and blood pressure is now a labeled concern as well 45. Sourcing testosterone online and injecting it without labs skips every one of these safety checks, which is how manageable risks turn into dangerous ones. There is no responsible version of TRT without blood testing. If a provider offers to skip it, that is a red flag, not a convenience. When you are ready, read our page on TRT side effects and the testosterone replacement therapy pillar to understand what proper monitoring looks like.
Is Andrew Huberman on TRT? What His Case Teaches About Target Levels
This sub-cluster ("huberman trt," "andrew huberman trt," "is andrew huberman on trt," "andrew huberman on trt," "huberman on trt," and "huberman lab trt") is worth answering factually, because it is a useful teaching case, not an endorsement. Andrew Huberman, the neuroscientist and podcast host, has publicly stated that he is on low-dose TRT, reportedly around 125 mg per week of testosterone cypionate started around age 45, and news coverage of his disclosures notes his level reportedly runs near 1,400 ng/dL on that protocol 12. He has also publicly urged caution, telling listeners to "wait, if you do it at all."
Here is the lesson, using his own reported numbers. A level near 1,400 ng/dL (about 48.6 nmol/L) is well above the guideline treatment target of mid-normal (roughly 450 to 600 ng/dL per the AUA, or 400 to 700 ng/dL mid-interval per the Endocrine Society) 12. That is an optimization or anti-aging choice, not the replacement target the evidence supports. Running levels that high pushes into supraphysiologic territory, where hematocrit rises and other risks increase, which is precisely the pattern the TRAVERSE safety data and the guidelines caution against 111. So the factual answer to "is Andrew Huberman on TRT" is that by his own account, yes, at a low dose, but his reported level is not a target to copy. There is no protocol to lift here, and the distinction between replacement and supraphysiologic dosing is exactly what our explainer on whether TRT is a steroid unpacks.
What If Your Levels Are Too High or Too Low
Once you are on therapy, two numbers can drift off target, and each has a signature and a fix. If your level is too high (above the upper end of normal, or frankly supraphysiologic), the tell is usually a rising hematocrit, which reaching about 52 to 54 percent is the threshold where clinicians act, along with acne, fluid retention, higher blood pressure, or disrupted sleep 145. The fix is a dose or frequency reduction, not adding more drugs to counteract the excess, and sometimes therapeutic phlebotomy for the hematocrit 111. High levels are corrected by dialing the dose down, not by stacking.
If your level is too low or your symptoms are not improving, the causes are usually a trough that falls too far before the next dose, an absorption or adherence issue with a gel, or a high SHBG that keeps too much testosterone bound. The answer is to recheck the timing and the dose with your prescriber rather than self-escalating 1. Persistent symptoms at a "normal" total testosterone are a reason to look at free testosterone and SHBG, not to assume more is always better. The management of both extremes is covered further in TRT side effects and TRT dosage.
Testosterone Levels on TRT for Women
Testosterone therapy in women is a different conversation with different numbers. Women make and need testosterone too, but the physiologic female range is a small fraction of the male range, so the target for any female testosterone therapy is far lower, typically delivered transdermally and titrated to keep levels within the normal female physiologic range rather than pushing into male or supraphysiologic territory 9. The labs and the interpretation differ accordingly. This page focuses on male replacement, so if you are researching female dosing and targets, see our dedicated guide to TRT for women.
Natural and Alternative Ways to Raise Testosterone
Not everyone who wants higher testosterone needs, or should start with, exogenous testosterone. The non-hype basics do help modestly: losing excess weight, improving sleep, resistance training, and treating conditions like untreated sleep apnea can each nudge natural production upward, and Mayo Clinic and Harvard both note lifestyle and underlying health as real contributors 910. These are not a substitute for treating genuine hypogonadism, but they are worth optimizing.
There are also prescription alternatives that raise your own production instead of replacing it, which matters if fertility is a concern. Because exogenous testosterone suppresses the body's own signaling and can reduce sperm production, some men use clinician-directed options such as enclomiphene or hCG, which stimulate endogenous testosterone while preserving fertility in a way that testosterone injections do not 12. Our guides to enclomiphene and hCG explain how those work, our overview of TRT alternatives compares the routes, and TRT and fertility covers why the fertility question should be settled before you start. What none of this includes is over-the-counter "testosterone boosters," which do not move these numbers meaningfully.
Frequently Asked Questions
There is no single perfect number, but the guideline target is the mid-normal range: the AUA describes treating to about 450 to 600 ng/dL (about 15.6 to 20.8 nmol/L), and the Endocrine Society aims for roughly 400 to 700 ng/dL (about 13.9 to 24.3 nmol/L) measured about a week after a weekly injection 12. The right level for you is the one that resolves your symptoms at the lowest effective dose, set by your clinician.
Yes. Exogenous testosterone raises both total and free testosterone, and because it can modestly lower SHBG, the free fraction often rises a little more than the total alone 6. Only about 1 to 3 percent of your testosterone is free, and that active fraction is what your tissues use.
By his own public statements, yes, at a low dose (reportedly about 125 mg per week of testosterone cypionate started around age 45), and news coverage notes his level reportedly runs near 1,400 ng/dL 12. That level is above the guideline replacement target and reflects an optimization choice rather than a target to copy 12.
The rule that matters most is consistency. For a weekly injection many clinics draw at trough (just before the next dose), while the Endocrine Society references a mid-interval reading about a week after the shot; gels are drawn a few hours after application once absorption is steady 14. Whatever point you choose, use it every time so results are comparable.
No. Diagnosis requires two morning total testosterone draws confirming a level below 300 ng/dL, and ongoing hematocrit and PSA monitoring is a safety requirement, not an optional extra 124. A provider willing to prescribe testosterone with no labs is a warning sign, because the monitoring is what keeps therapy safe.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432 (amended).
- Travison TG, et al. Harmonized Reference Ranges for Circulating Testosterone Levels in Men of Four Cohort Studies in the US and Europe. J Clin Endocrinol Metab. 2017;102(4):1161-1173.
- U.S. Food and Drug Administration. AndroGel 1.62% (testosterone gel) Prescribing Information. 2016.
- U.S. Food and Drug Administration. FDA issues class-wide labeling changes for testosterone products. February 2025.
- MedlinePlus. Testosterone Levels Test. U.S. National Library of Medicine. Accessed 2026.
- Cleveland Clinic. Low Testosterone (Male Hypogonadism). Accessed 2026.
- Cleveland Clinic. Testosterone Test. Accessed 2026.
- Mayo Clinic. Testosterone therapy: Potential benefits and risks as you age. Accessed 2026.
- Harvard Health Publishing. Testosterone: What it does and doesn't do. Accessed 2026.
- Lincoff AM, Bhasin S, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023;389(2):107-117.
- Futurism. Andrew Huberman's TRT disclosure (news coverage). Accessed 2026.
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.