TRT alternatives fall into three honest groups: prescription medicines that raise your own testosterone (SERMs like enclomiphene and clomiphene, plus hCG), lifestyle changes that reverse a fixable cause, and support supplements you take alongside testosterone rather than instead of it. Whether any of these can actually replace testosterone replacement therapy hinges on one question almost every article skips: is your low testosterone primary (the testicles have failed) or secondary (the testicles work, but the signal from the brain is low)? That single distinction decides everything on this page. In secondary low T, alternatives can restart your body's own production. In primary low T, nothing but TRT raises testosterone. Below we walk through what raises testosterone, what only supports you while on TRT, and what is mostly marketing, with each claim anchored to Endocrine Society, AUA, and clinic-level evidence rather than gym-floor rumor.
Key Takeaways
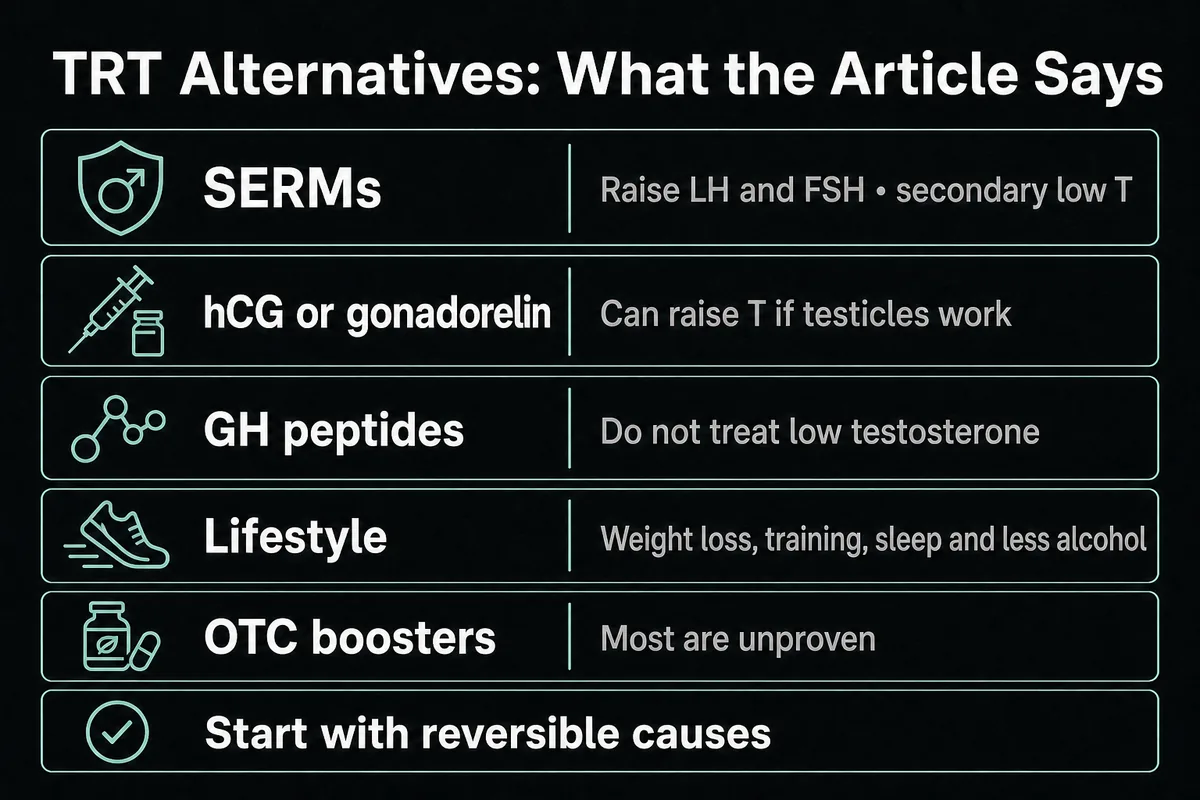
- The primary-vs-secondary split governs everything. SERMs, hCG, and weight loss can raise testosterone only when the testicles still work and the problem is upstream (secondary). In primary testicular failure, TRT is the only option that raises T 125.
- SERMs are the leading prescription alternative. Across randomized trials, clomiphene or enclomiphene raised total testosterone by roughly 273 ng/dL versus placebo in secondary or functional hypogonadism, and unlike TRT they preserve fertility 7.
- Growth-hormone peptides do not treat low testosterone. Sermorelin, CJC-1295, and ipamorelin act on the growth hormone axis, not the testosterone axis, so they are stacked with TRT for sleep and recovery, not used as a replacement 16.
- The only peptides that raise T are gonadotropins. hCG and gonadorelin drive the testosterone axis directly and can raise T if the testicles function 9.
- Most OTC "testosterone boosters" are unproven. In one analysis of popular online boosters, only about 24.8 percent had any data showing a testosterone increase, and about 10.1 percent showed a decrease 1011.
- Lifestyle first is the guideline stance. Treating reversible causes, especially excess weight, is where clinicians start, and it can meaningfully raise testosterone in overweight and sedentary men 151415.
TRT alternatives at a glance
There are two very different reasons people search for TRT alternatives, and this page answers both. Some men want something instead of testosterone, often to protect fertility or avoid a lifelong prescription. Others are already on TRT and want a support stack to feel their best. The honest bottom line up front: a small set of prescription medicines (the SERMs enclomiphene and clomiphene, plus hCG) can raise your own testosterone, but only when your low T is secondary and your testicles still work 67. Lifestyle change, above all weight loss, is the highest-yield natural lever and the one guidelines tell clinicians to try first 15. Supplements, whether OTC boosters or a support stack, do not replace TRT, and most boosters have little evidence behind them 1011. Everything downstream depends on the fork we cover next.
First, the fork: why some alternatives to TRT only work for some men
Before you compare any options, you need to know which kind of low testosterone you have, because it changes which alternatives to TRT are even possible. This is the step nearly every ranking page omits, and it is the difference between a plan that can work and one that cannot.
Primary vs secondary hypogonadism (the fact that decides everything)
Testosterone is made by the testicles on orders from the brain. The pituitary sends luteinizing hormone (LH) and follicle-stimulating hormone (FSH), and the testicles respond by producing testosterone and sperm 2.
In secondary hypogonadism, the testicles are capable, but the signal from the brain is low. Here the axis can be restarted: SERMs raise LH and FSH, hCG mimics LH, and losing weight can lift the body's own production 567. Alternatives to TRT genuinely exist for these men.
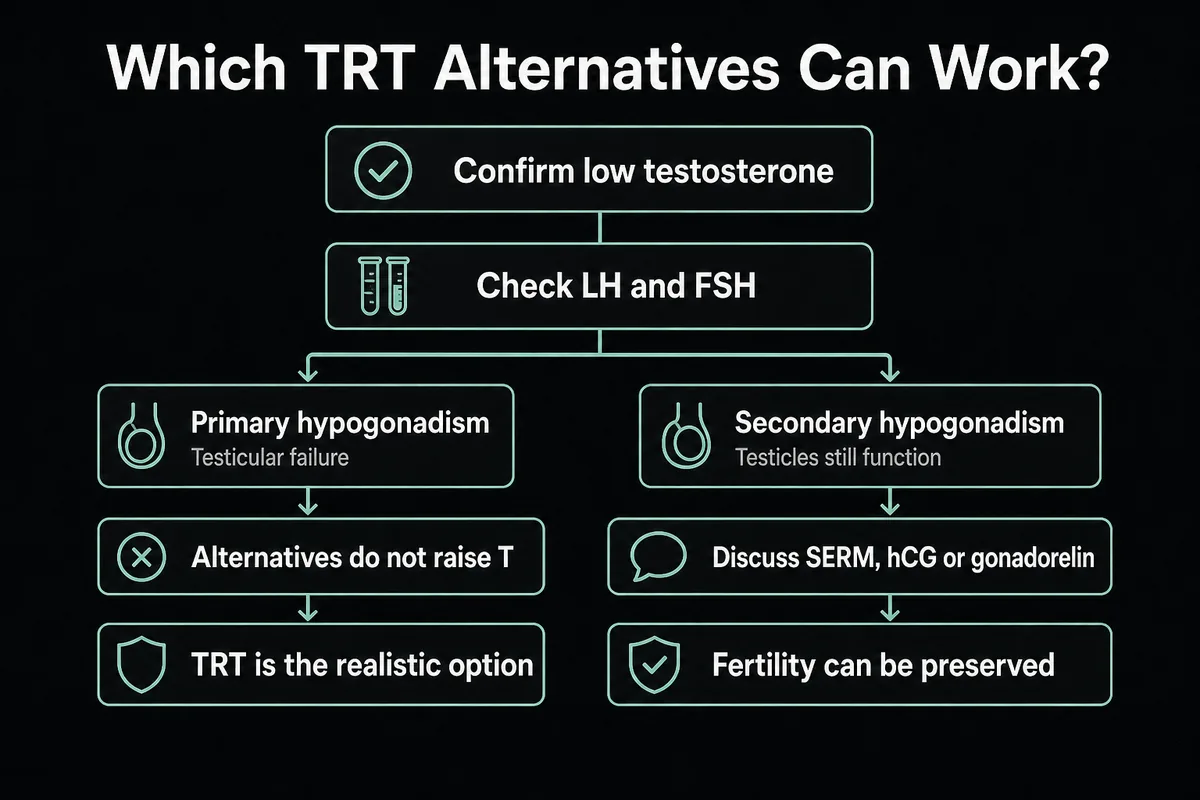
In primary hypogonadism, the testicles themselves have failed and cannot respond no matter how loud the signal. SERMs and hCG do little to nothing, and TRT is the only treatment that raises testosterone 2. Because the two look identical from symptoms alone, your clinician confirms which you have with a repeat morning testosterone test plus LH and FSH labs before choosing a path 12. Treating reversible causes first, and counseling men on fertility, is the explicit position of both the Endocrine Society and the AUA 134. If you may want children, this is also the moment to flag it, because it steers you toward fertility-sparing options covered in our guide to TRT and fertility.
Prescription alternatives to TRT that actually raise testosterone
For men with secondary low T, a handful of prescription medicines can raise testosterone without adding testosterone from outside the body. Because they work through your own axis, they generally preserve fertility, which is the single biggest advantage over TRT 69. All of them are physician-directed, and none of them work in primary testicular failure.
Enclomiphene (a SERM that restarts your own testosterone)
Enclomiphene is a selective estrogen receptor modulator (SERM). It blocks estrogen feedback at the brain, so the pituitary releases more LH and FSH, and the testicles make more testosterone 6. In reviews of secondary male hypogonadism, enclomiphene raised testosterone into the normal range while preserving semen parameters, making it an option when TRT is unsuitable or when fertility matters 6. It is taken as a daily oral tablet rather than an injection or gel. Because it depends on working testicles, it does nothing for primary failure. Our detailed enclomiphene guide covers how it is dosed and monitored.
Clomiphene citrate (Clomid) as a testosterone alternative
Clomiphene citrate (brand name Clomid) is the older, closely related SERM, and it is used off-label in men for the same reason: it raises LH and FSH and, in turn, testosterone 8. The Cleveland Clinic specifically notes clomiphene as an option for men who want to preserve fertility 5. Enclomiphene is essentially the purified active isomer of clomiphene, which is why the two behave similarly. The pooled evidence is encouraging: a systematic review and meta-analysis of randomized trials found that clomiphene or enclomiphene raised total testosterone by about 273.76 ng/dL versus placebo, and importantly, that benefit applied to secondary or functional hypogonadism, with primary hypogonadism excluded 7. Clomiphene can occasionally cause visual or mood side effects, so it is a monitored prescription, not a self-managed supplement.
hCG, the main hcg alternative for TRT question, answered
Human chorionic gonadotropin (hCG) works differently from the SERMs. Rather than nudging the brain, it acts like LH and stimulates the testicles directly to make testosterone and to maintain sperm production 9. That makes it useful in two settings: as a standalone option for some men with secondary low T, and as an add-on to preserve intratesticular testosterone and fertility in men who are on TRT 9. So the common "what is a good hCG alternative for TRT" question usually flips around: hCG is itself one of the main fertility-sparing tools, and the SERMs above are the oral alternatives to it. As with the others, hCG needs functioning testicles to work. See our hCG explainer for mechanism and use.
Gonadorelin and other gonadotropin options
Gonadorelin is a synthetic form of gonadotropin-releasing hormone (GnRH), the upstream signal that tells the pituitary to release LH and FSH. Given in the right pulsed way, it can stimulate the axis and is sometimes used as a gonadotropin-style option or add-on 2. Like the SERMs and hCG, it depends on an intact downstream system. The table below sums up how these prescription alternatives compare with TRT itself.
Table 1. Prescription alternatives to TRT
| Option | How it works | Raises your own T? | Preserves fertility? | Best for | Status |
|---|---|---|---|---|---|
| Enclomiphene | SERM, raises LH and FSH | Yes (secondary only) | Yes | Secondary low T wanting fertility | Rx |
| Clomiphene (Clomid) | SERM, raises LH and FSH | Yes (secondary only) | Yes | Secondary low T, off-label | Rx |
| hCG | LH analog, drives testes | Yes (if testes work) | Yes | Fertility, or add-on to TRT | Rx |
| Gonadorelin | GnRH analog, pulses LH and FSH | Yes (secondary only) | Yes | Axis stimulation, add-on | Rx |
| TRT | Exogenous testosterone | No (replaces it) | No (suppresses sperm) | Primary failure or when others fail | Rx (Schedule III) |
TRT itself sits in the last row for a reason: it replaces testosterone rather than raising your own, and by design it suppresses the axis and sperm production 918. That trade-off is why so many men look at the rows above it. For a fuller picture of what TRT delivery looks like, see types of TRT.
Peptides vs TRT: do TRT peptides raise testosterone?
This is the most confused corner of the whole topic. Search results for "peptides vs trt" and "trt peptides" are dominated by muscle-and-recovery pages that blur two completely different drug classes. Here is the honest, mechanism-based verdict.
Growth-hormone peptides (sermorelin, CJC-1295, ipamorelin) are not a testosterone treatment
The peptides most people mean by "TRT peptides" (sermorelin, CJC-1295, ipamorelin, and tesamorelin) are growth hormone secretagogues. They prompt the body to release more growth hormone, which raises IGF-1. They act on the growth hormone and IGF-1 axis, not the testosterone axis, so they do not treat low testosterone 16. Men use them for sleep quality, recovery, and body composition, which is a real but separate goal. If your problem is low T, a growth-hormone peptide will not fix it, and framing it as a TRT replacement is the central error in most "trt vs peptides" content.
The only peptides that raise testosterone (gonadotropins: hCG, gonadorelin)
The one peptide class that does raise testosterone is the gonadotropin group covered earlier: hCG and gonadorelin. They act on the testosterone (HPG) axis, so they can raise T when the testicles work, and they are the peptides used for fertility, axis restart, or as a TRT add-on 9. If someone tells you a peptide "raises testosterone," it is almost certainly one of these, not a growth-hormone secretagogue.
Sermorelin with TRT and the best peptide to take with TRT
So what about running sermorelin with TRT, and what is the best peptide to take with TRT? The realistic answer is that these are complements, not replacements. Men run sermorelin and TRT together to support sleep and recovery while TRT handles the testosterone side, which matches what users consistently report. If the goal is specifically to support testosterone and fertility on TRT, the peptide that matters is hCG, not a growth-hormone secretagogue 9. Our comparison hub on sermorelin vs TRT breaks these down side by side.
Table 2. Peptides vs TRT
| Approach | Axis it acts on | Raises testosterone? | Typical use | Evidence for low T |
|---|---|---|---|---|
| TRT | Testosterone (HPG) | Yes (replaces) | Diagnosed hypogonadism | Established |
| Sermorelin / CJC-1295 / ipamorelin | GH / IGF-1 | No | Sleep, recovery, body composition | Not a low-T treatment |
| Tesamorelin | GH / IGF-1 | No | Visceral fat (FDA approved for HIV lipodystrophy) | Not a low-T treatment |
| hCG / gonadorelin | Gonadotropin (HPG) | Yes (if testes work) | Fertility, restart, TRT add-on | Established |
Are "testosterone boosters" a real TRT alternative? What the evidence says
Walk into any supplement shop and you will see shelves of "testosterone boosters." Almost none are a real alternative to TRT, and the data on them is unflattering. It is worth remembering the broader caution here: even for prescription testosterone, marketing has tended to outpace the evidence, which is exactly why sober, guideline-anchored framing matters 17.
What is a TRT supplement (and what OTC boosters actually do)
The phrase "TRT supplement" gets used for two different things. One is the OTC "testosterone booster," a pill blend marketed to raise your testosterone. The other is a support supplement (vitamin D, magnesium, omega-3) taken to support general health while on prescription TRT, covered in the next section. They are not interchangeable, and neither replaces a medical low-T diagnosis. On the booster side, the evidence is weak: in an analysis of popular online testosterone boosting supplements, only about 24.8 percent had any data showing a testosterone increase, about 10.1 percent showed a decrease, and many showed no change 10. A separate review concluded that the composition and marketing claims of these products are not supported by the academic literature, with a majority of common ingredients carrying weak evidence 11. In short, most OTC boosters are buyer-beware, not a TRT alternative.
Ashwagandha and TRT: the one herb with modest evidence
Ashwagandha is the honest exception worth naming. In a systematic review of herbs and testosterone, ashwagandha was among the few ingredients with any positive signal, while most were unproven 12. In one randomized crossover trial in aging, overweight men, ashwagandha was associated with roughly a 15 percent increase in testosterone, though the change stayed within the normal range 13. That is a modest effect in men who are not on TRT, and it is not a substitute for treating diagnosed hypogonadism. If you already take TRT, ashwagandha is generally used for stress and sleep, and any supplement should be cleared with your prescriber first.
Best supplements to take while on TRT (the support stack)
If you are already on TRT, the useful question is not "what raises my testosterone" (TRT is doing that) but "what supports my overall health and corrects real deficiencies." That reframing is the whole point of a support stack. The best supplements to take while on TRT are the ones that fix a genuine shortfall or support sleep, recovery, and cardiometabolic health, not the ones marketed to spike testosterone.
Vitamin D, magnesium, zinc, omega-3, boron
The consensus support stack is modest and evidence-anchored: correct a low vitamin D level, cover common magnesium and omega-3 shortfalls, and supplement zinc only if you are actually deficient. Vitamin D is the standout because so many men run low, and it supports overall health rather than acting as a testosterone drug 12. Magnesium supports sleep and muscle function, omega-3 supports cardiometabolic health, and boron and creatine have limited or mixed roles in recovery and performance. None of these is a testosterone treatment on top of TRT, and framing them that way oversells them.
Table 3. Support supplements while on TRT
| Supplement | What it supports | Evidence | Note |
|---|---|---|---|
| Vitamin D3 | Correcting deficiency, overall health | Moderate | Test your level, many men run low |
| Magnesium | Sleep, muscle, deficiency | Moderate | Common dietary shortfall |
| Omega-3 | Cardiometabolic health | Moderate | Diet-dependent |
| Zinc | Only if deficient | Weak on TRT | Do not megadose |
| Boron / creatine | Recovery, performance | Mixed or limited | Not T-raising on TRT |
| OTC "T booster" blends | Marketed as T-raising | Poor (about 25 percent show any effect) | Generally skip 10 |
What to skip: supplements to avoid stacking with TRT
The "what to skip" list matters as much as the take list. Piling on extra zinc when you are not deficient adds little and can crowd out copper. Stacking DHEA on top of TRT is usually redundant. And products that promise to control estrogen or "block aromatase" over the counter are best avoided, because managing estradiol on TRT is a lab-guided, physician-directed decision, not a supplement one, as we discuss in TRT side effects. The general rule: a support stack corrects deficiencies and supports health, it does not fine-tune your hormones, and anything aimed at hormone tuning belongs with your clinician. For the fuller booster-versus-peptide comparison, see testosterone boosters vs peptides.
Lifestyle alternatives that raise testosterone naturally
Lifestyle change is not a consolation prize. For many men with borderline or obesity-related low T, it is the highest-yield lever available, and it is exactly what guidelines mean when they say to treat reversible causes first 15. It will not fix true primary testicular failure, but it can move the needle meaningfully in the men it applies to.
Weight loss (the highest-yield lever for many men)
Excess body fat lowers testosterone, and losing weight can reverse a good part of obesity-related low T. A review of BMI and testosterone found that reductions in weight and BMI are associated with higher serum testosterone 14. Because obesity is one of the most common reversible causes, weight loss is often the first thing a clinician addresses, and for some men it raises testosterone enough that no medication is needed. Our guide to TRT and weight loss covers how the two interact.
Resistance training, sleep, and alcohol
Exercise adds to the effect. A systematic review and meta-analysis found that aerobic exercise training raised testosterone concentration in individuals who were obese or had type 2 diabetes 15, and resistance training supports the same direction, especially in sedentary men. Sleep and alcohol round out the picture: chronically short sleep and heavy drinking both suppress testosterone, so protecting sleep and moderating alcohol are simple, no-downside levers. None of this is hype, and none of it replaces treatment for primary failure, but for the right man it is genuinely a real alternative to TRT.
"Is The Rock on TRT?" and the legal TRT alternative question
Curiosity keywords like "is The Rock on TRT" deserve a straight answer rather than gossip. We cannot and will not diagnose or speculate about any individual, and no honest article can. What we can address is the real question underneath it: is there a legal TRT alternative you can buy that equals prescription testosterone? The answer is no. There is no legal over-the-counter product equivalent to prescription testosterone. SARMs, which are often marketed this way, are unapproved and illegal to sell for human use, and they are not a safe or legitimate substitute. The only legitimate "legal TRT alternatives" are the prescription SERMs and hCG for the right candidate (secondary low T) or the lifestyle changes above 1011. For the specific legal rules, see is TRT legal.
How to choose an alternative to TRT (decision guide)
Choosing an alternative to TRT is not a menu pick, it is a decision made with your clinician after labs. The short version keyed to the fork:
- Get diagnosed first. Confirm low testosterone on a repeat morning test and get LH and FSH to separate primary from secondary 12.
- Primary (testicular failure): alternatives do not raise T, so TRT is the realistic option, and the choice is about delivery, not whether 2.
- Secondary, and you want fertility: enclomiphene, clomiphene, or hCG are the fertility-sparing options to discuss 567.
- Overweight or sedentary: treat that first, because weight loss and training may raise your own testosterone without medication 1415.
- Already on TRT: think support stack (correct deficiencies), not more testosterone boosters, and consider whether age and goals still favor treatment, as covered in best age for TRT and TRT vs HRT.
Every path here is physician-directed. If you are considering coming off testosterone toward an alternative, do it as a planned taper, not a sudden stop, as we explain in stopping TRT.
Frequently Asked Questions
The term covers two different things. One is an OTC "testosterone booster" marketed to raise your testosterone, which is mostly unproven 1011. The other is a support supplement (vitamin D, magnesium, omega-3) taken to support health while on prescription TRT 12. Neither replaces a medical low-T diagnosis.
Ashwagandha is generally used for stress and sleep. It has modest evidence for a small testosterone rise in men not on TRT (about 15 percent in one trial), but it does not replace TRT 13. Clear any supplement with your prescriber first.
We cannot diagnose or speak for any individual. Broadly, there is no legal over-the-counter product equal to prescription testosterone, SARMs are unapproved and illegal to sell for human use, and the only legitimate legal alternatives are prescription SERMs or hCG for the right candidate, or lifestyle change 1011.
The bottom line
TRT alternatives are real, but only within limits the marketing rarely admits. They exist mainly for secondary hypogonadism, where SERMs (enclomiphene, clomiphene) and hCG can raise your own testosterone and spare fertility, and where losing weight and training can lift levels naturally 5671415. Growth-hormone peptides like sermorelin are not a testosterone treatment, they are a complement for sleep and recovery 16. OTC testosterone boosters are mostly unproven, and support supplements support your health rather than replacing treatment 101112. In primary testicular failure, none of this raises testosterone, and TRT remains the only option 2. The move that matters most is the first one: get diagnosed, separate primary from secondary with LH and FSH, and choose a path with your clinician 13. Start with our pillar on testosterone replacement therapy, then explore enclomiphene, hCG, and TRT and fertility to go deeper on the fertility-sparing options.
References
- Endocrine Society. Testosterone Therapy for Hypogonadism Clinical Practice Guideline. Accessed 2026.
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- American Urological Association. Testosterone Deficiency Guideline. Accessed 2026.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018.
- Cleveland Clinic. Low Testosterone (Male Hypogonadism). Accessed 2026.
- Wheeler KM, et al. Enclomiphene Citrate for the Treatment of Secondary Male Hypogonadism. Sex Med Rev. 2019.
- Clomiphene or enclomiphene citrate for the treatment of male hypogonadism: a systematic review and meta-analysis of RCTs. PMC. 2024.
- Clomiphene citrate: A potential alternative for testosterone therapy in hypogonadal males. PMC. 2023.
- Crosnoe LE, Grober E, Ohl D, Kim ED. Exogenous testosterone: a preventable cause of male infertility. Transl Androl Urol. 2013.
- Balasubramanian A, et al. Testosterone Imposters: An Analysis of Popular Online Testosterone Boosting Supplements. World J Mens Health. 2019.
- 'Testosterone Boosting' Supplements Composition and Claims Are Not Supported by the Academic Literature. World J Mens Health. 2020.
- Smith SJ, et al. Examining the Effects of Herbs on Testosterone Concentrations in Men: A Systematic Review. Adv Nutr. 2021.
- Lopresti AL, et al. A Randomized, Double-Blind, Placebo-Controlled, Crossover Study Examining the Hormonal and Vitality Effects of Ashwagandha in Aging, Overweight Males. Am J Mens Health. 2019.
- Impact of Weight Loss on Testosterone Levels: A Review of BMI and Testosterone. PMC. 2024.
- The Effects of Aerobic Exercise Training on Testosterone Concentration in Individuals Who are Obese or Have Type 2 Diabetes: A Systematic Review and Meta-Analysis. PMC. 2024.
- Mayo Clinic. Testosterone therapy: Potential benefits and risks as you age. Accessed 2026.
- Harvard Health Publishing. Is testosterone therapy safe? Take a breath before you take the plunge. Accessed 2026.
- U.S. Food and Drug Administration. AndroGel (testosterone gel) Prescribing Information. 2025.
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.