TRT and prostate cancer is one of the oldest worries in men's health, and the short answer is reassuring: for men with confirmed low testosterone, current evidence does not show that TRT causes prostate cancer. The genuine cautions are narrower and specific. A prostate cancer that already exists is testosterone-sensitive and can be fed by it, so active or untreated disease is a reason to avoid testosterone. A rise in PSA needs a proper workup rather than a shrug. And starting therapy after a prostate cancer history is a careful, specialist-led decision, not a routine one. This page answers the three questions the search results usually split apart, does testosterone therapy cause prostate cancer, is it safe after prostate cancer, and does it worsen an enlarged prostate, against Endocrine Society, AUA, and FDA guidance rather than gym-floor rumor. Testosterone is a prescription, controlled medication, so every candidacy and monitoring point here is one your clinician decides with you. For the fuller picture of treatment, see our pillar guide to testosterone replacement therapy.
Key Takeaways
- No strong evidence TRT causes new prostate cancer: in men with documented low testosterone, large trial and medical-center data do not show that properly dosed TRT triggers new prostate cancer 367.
- Existing prostate cancer is the real concern: an established prostate tumor is often androgen-dependent, which is why active or untreated disease is a contraindication, not a monitoring problem 56.
- The saturation model explains why: prostate androgen receptors are already saturated at low testosterone levels, so once a man is above that threshold, adding more testosterone adds little prostate stimulation 4.
- PSA and a prostate exam come before and during: a baseline PSA plus a digital rectal exam, then scheduled rechecks, are how clinicians catch a meaningful change early 12.
- TRT after prostate cancer is a specialist shared decision: cautious, supervised use is possible in carefully selected survivors, but long-term data are limited, so it is case-by-case 911.
- TRT does not appear to worsen an enlarged prostate: it may raise prostate volume slightly but does not seem to worsen urinary symptoms in most men 10.
Does TRT cause prostate cancer?
For men with documented low testosterone, there is no strong evidence that TRT causes new prostate cancer. This is the current position of major cancer centers and the largest dedicated trial to date. Mayo Clinic states plainly that naturally occurring testosterone is not likely to raise a person's risk of developing prostate cancer, and that appropriately used testosterone therapy for men with low levels does not appear to increase that risk 6. MD Anderson reaches the same conclusion and adds that there is no clear correlation showing that a particular testosterone level places a man at higher risk of prostate cancer 8.
The fear traces back to old observations that lowering testosterone can shrink an existing tumor, which led to a decades-long assumption that raising testosterone must do the reverse. That assumption has not held up under modern study. The important distinction, which the rest of this page keeps drawing, is between causing a new cancer (not supported by the evidence) and feeding a cancer that is already present (a real effect, and the reason active disease is a contraindication).
What the research actually shows
The strongest recent evidence comes from the TRAVERSE trial's prostate-safety sub-study, published in JAMA Network Open in 2023. Among 5,204 middle-aged and older men with low testosterone and elevated cardiovascular risk, followed across more than 14,000 person-years, high-grade prostate cancer occurred in 0.19 percent of the testosterone group versus 0.12 percent of the placebo group, a difference that was not statistically significant 3. Any prostate cancer occurred in 0.46 percent versus 0.42 percent, again not significant 3. Rates of acute urinary retention, invasive prostate procedures, and new medication for benign prostate enlargement were also similar between the groups 3.
Put in absolute terms, these are small fractions of one percent in both arms, and the study found no signal that testosterone therapy meaningfully raises prostate cancer risk over the trial period. A separate analysis reported by Harvard Health, drawn from a JAMA Network Open study of 5,246 hypogonadal men, likewise found no increase in prostate cancer risk versus placebo, with only a small PSA rise in the first year that then stabilized 7. Neither study is a promise of zero risk, and both enrolled screened men, but together they are the best available answer to whether TRT causes prostate cancer.
The saturation model: why more testosterone is not more risk
The mechanism behind these findings has a name: the saturation model, described by Morgentaler and Traish in European Urology in 2009 4. Prostate tissue responds to androgens through a fixed number of androgen receptors, and those receptors become fully occupied, or saturated, at relatively low testosterone concentrations, near the castrate range 4. Below that point, adding testosterone does drive prostate growth. Above it, the receptors are already full, so extra testosterone produces little additional prostate stimulation 4.
This is why the old one-to-one belief, that more testosterone must mean more prostate cancer, was overturned. Most men considering TRT already have testosterone above the saturation threshold even when their levels feel low, so raising a low-normal level toward mid-normal does not flood the prostate with new growth signal. The saturation model is the clearest explanation for why the trials keep finding no meaningful risk increase.
Can TRT cause cancer more broadly?
Stepping back from the prostate, testosterone does not appear to increase overall cancer risk. MD Anderson frames it directly: testosterone does not increase cancer risk, and the reason androgen-deprivation therapy works against prostate cancer is that it removes a growth signal from a tumor that is already there, not that testosterone plants new tumors 8. The prostate is simply a testosterone-sensitive tissue, in the same way breast tissue is estrogen-sensitive. Hormone sensitivity means an existing cancer in that tissue can be fueled by the hormone, which is a different statement from saying the hormone starts the cancer.
At replacement doses, TRT is not established as a cause of cancers elsewhere in the body. The prostate gets attention because of its clear androgen dependence, and male breast cancer is the other hormone-sensitive tissue listed on testosterone labels as a contraindication 512. Outside those specific situations, the concern with TRT and cancer is not a general one. Supraphysiologic misuse well above replacement levels is a separate world from monitored therapy, with a risk profile this page does not endorse.
Table 1. Myth versus evidence: TRT and the prostate
| Claim | What the evidence shows | Source type |
|---|---|---|
| TRT causes prostate cancer | No strong evidence in men with documented low testosterone; contraindicated only when a cancer already exists 367 | Large RCT plus cancer-center reviews |
| More testosterone means more prostate cancer | The saturation model: prostate receptors are saturated at low testosterone, so extra testosterone adds little stimulation 4 | Urology research |
| TRT worsens an enlarged prostate | May raise prostate volume slightly but does not appear to worsen urinary symptoms in most men 10 | Review of 35 studies |
| You can never have TRT after prostate cancer | Cautious, specialist-supervised use is possible in selected survivors, though long-term data are limited 911 | Scoping review plus clinic guidance |
| TRT raises PSA a lot | Usually a small rise in the first months, then it stabilizes 17 | Guideline plus trial |
TRT and existing prostate cancer: why active disease is different
Everything above applies to men who do not already have prostate cancer. When a cancer is present, the calculus flips, and this is where TRT and prostate cancer stop being reassuring. Most prostate cancers are androgen-dependent, meaning they use testosterone as fuel for growth. This is not theoretical; it is the basis of a standard treatment. Androgen-deprivation therapy deliberately lowers testosterone to starve prostate tumors, and it works because it removes the growth signal 8.
For that reason, giving testosterone to a man with active, untreated, or metastatic prostate cancer runs against the biology, and it is a clear contraindication. FDA prescribing information states that testosterone products are contraindicated in men with known or suspected carcinoma of the prostate 5, consumer drug labeling repeats the warning 12, and Cleveland Clinic lists prostate cancer among the conditions that make TRT unsafe 9. The line to hold in mind: TRT does not appear to create prostate cancer, but it can accelerate one that is already there, which is why screening before you start matters as much as monitoring afterward. Prostate changes are one reason PSA sits on the standard TRT side effects monitoring panel.
TRT after prostate cancer: is it safe?
TRT after prostate cancer is the fastest-changing part of this topic. Historically, any man with a prostate cancer history was told to avoid testosterone permanently, on the theory that even a treated cancer might harbor cells waiting for fuel. That blanket rule is softening. A 2025 scoping review in the International Journal of Impotence Research concluded that, although the question remains controversial, the assembled evidence supports cautious use of TRT in carefully selected men after curative prostate cancer treatment, while noting that long-term safety data are still limited 11. Cleveland Clinic similarly notes that TRT may be an option after successfully treated prostate cancer, with close PSA monitoring 9.
Importantly, the AUA guideline does not hand out a green light. It states that for men with a history of prostate cancer, there is inadequate evidence to quantify the risk-benefit balance, so the decision becomes a shared one between the man and his specialists 2. That is the honest framing: not safe as a blanket claim, not forbidden as a blanket claim, but an individualized decision made with a urologist or oncologist who knows the specifics of the cancer that was treated.
Candidacy after radical prostatectomy vs radiation
Candidacy is not one-size-fits-all, and the type of treatment a man had changes how his PSA is read. After a radical prostatectomy (surgical removal of the prostate), PSA should fall to undetectable, because the tissue that makes it is gone, so a truly undetectable and stable PSA is the reassuring signal clinicians look for before considering TRT 911. After radiation, the prostate stays in the body, so PSA does not fall to zero; it settles to a low nadir, and clinicians track for a rise above that nadir instead. That difference matters, because a number that would be alarming after surgery can be normal after radiation.
Beyond the PSA picture, the men most often considered have low-risk, curatively treated disease, a stable or undetectable PSA, and typically a waiting period (often one to two years) after treatment before testosterone is introduced, all under urology or oncology oversight 11. None of this is a do-it-yourself protocol. Prostate history is also part of why the best age for TRT conversation looks different for older men, who carry more baseline prostate risk to weigh.
TRT after testicular cancer
TRT after testicular cancer is a different situation and should not be lumped in with prostate cancer. Testicular cancer is not androgen-driven, so testosterone does not fuel it the way it can prostate tumors. Its treatments, including removal of a testicle (orchiectomy) and chemotherapy, frequently cause low testosterone by damaging the body's ability to make it. In that setting, TRT is commonly used to treat the resulting deficiency rather than being avoided. The concern that governs prostate cancer decisions does not carry over, though the decision still belongs with the treating oncology team, based on recovery and hormone levels.
Table 2. TRT and prostate cancer: safe, caution, or avoid
| Situation | TRT status | Why |
|---|---|---|
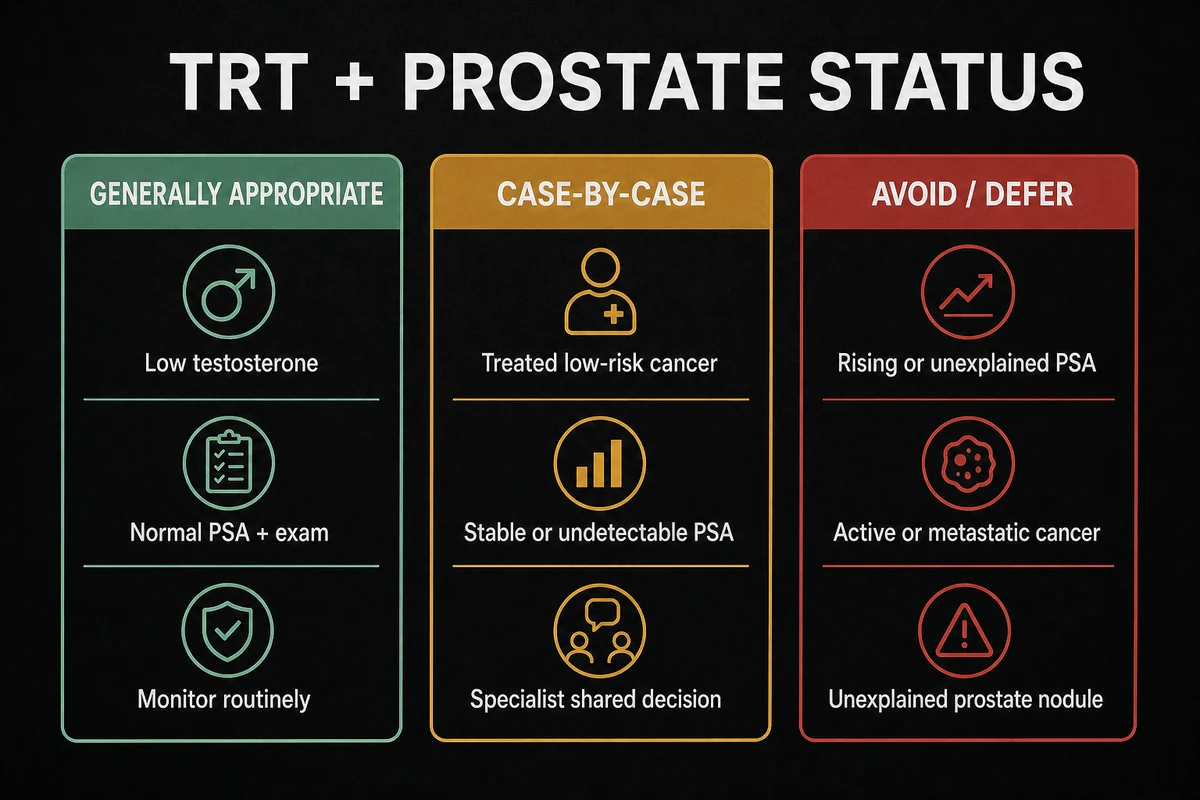
| Documented low testosterone, normal PSA and prostate exam | Generally appropriate with monitoring | No evidence TRT causes new prostate cancer in this group 16 |
| Treated low-risk cancer, undetectable or stable PSA | Case-by-case, specialist shared decision | Growing but limited evidence supports cautious, supervised use 911 |
| Rising or unexplained PSA | Avoid pending workup | A PSA change must be evaluated before starting or continuing 1 |
| Active, untreated, or metastatic prostate cancer | Contraindicated | Existing prostate cancer is testosterone-sensitive 56 |
| Palpable prostate nodule or induration | Avoid until evaluated | Guidelines advise against TRT until the finding is worked up 1 |
| After testicular cancer with low testosterone | Commonly used to treat the deficiency | Testicular cancer is not androgen-driven 9 |
TRT and enlarged prostate (BPH)
Separate from cancer, many men ask whether TRT worsens an enlarged prostate, or benign prostatic hyperplasia (BPH), the common non-cancerous prostate growth that causes urinary symptoms with age. The honest answer distinguishes prostate volume from prostate symptoms. Testosterone may modestly increase prostate volume, but that does not reliably translate into worse urinary symptoms for most men. A University of Illinois review of 35 studies, summarized by the Sexual Medicine Society of North America, found that in men with mild lower urinary tract symptoms, those symptoms either improved or stayed unchanged after starting TRT 10. The same source notes that roughly half of men in their fifties already have an enlarged prostate, which puts the question in perspective: BPH is extraordinarily common with or without testosterone therapy 10.
The fair caveat is that many of these studies excluded men with severe urinary symptoms, so the reassurance is strongest for mild-to-moderate BPH and less certain for men with significant obstruction 10. If you already have bothersome urinary symptoms, flag them to your clinician before starting, because your baseline symptoms will be monitored along the way. For most men, though, TRT and prostate enlargement is not the automatic problem it is sometimes made out to be.
PSA monitoring on TRT: what to expect
PSA (prostate-specific antigen) is the blood marker that anchors prostate safety on TRT, and knowing how it behaves prevents needless alarm. Expect a small PSA rise in the first three to six months as testosterone normalizes, then a plateau; the Harvard-reported study saw exactly this pattern, a modest first-year rise followed by stabilization 7. A small early bump is a normal response, not a red flag on its own.
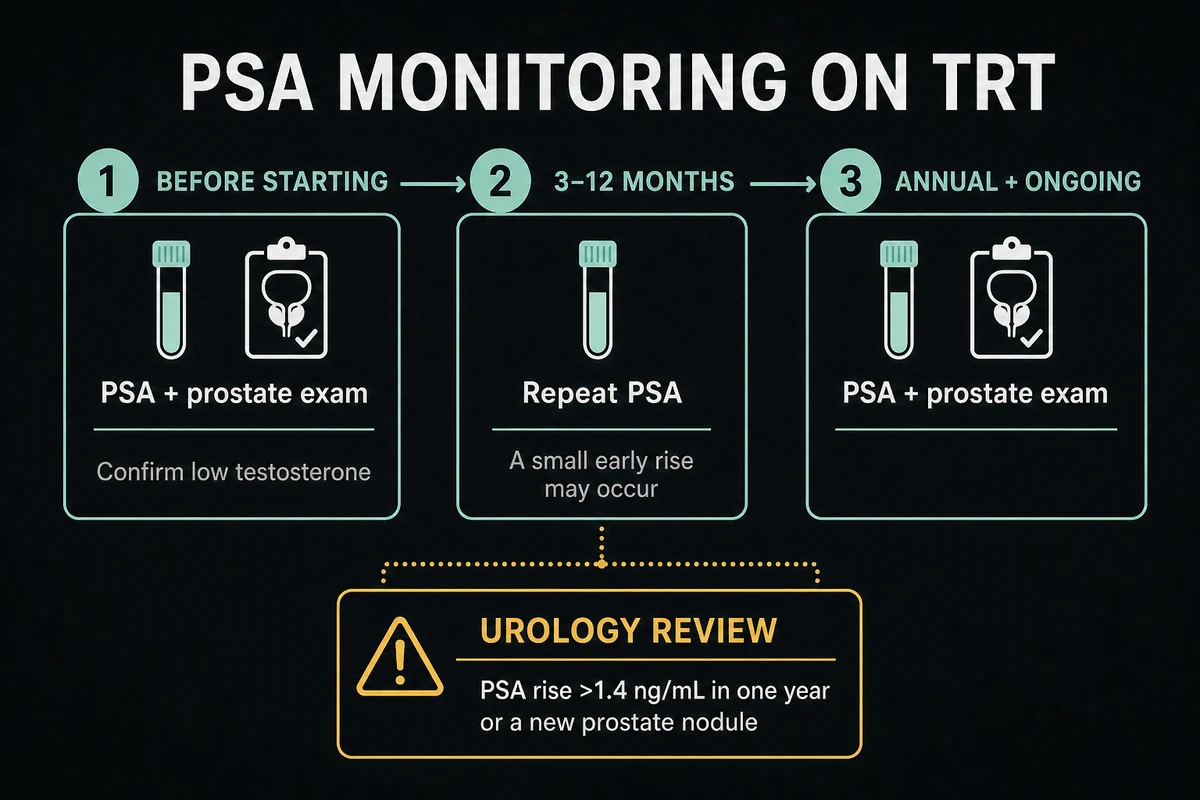
What clinicians watch for is a change beyond that expected settling. Guidance flags a confirmatory workup when PSA rises by more than about 1.4 ng/mL within a single year, or when the absolute PSA crosses a threshold that warrants urology review 1. The Endocrine Society recommends measuring PSA and performing a digital rectal exam before starting testosterone in men at risk, then rechecking PSA between three and twelve months after starting, and periodically thereafter 1. The AUA similarly advises a baseline PSA in men over 40 before beginning therapy 2. A meaningful rise or a new abnormal exam prompts referral, not an automatic cancer diagnosis. Because PSA is read alongside your testosterone results, the two are tracked together, which is covered further in our guide to testosterone levels on TRT.
Table 3. PSA monitoring timeline on TRT
| Timepoint | Test | What it flags |
|---|---|---|
| Baseline (before starting) | PSA plus digital rectal exam plus confirmed low testosterone | Screens for existing prostate disease before therapy begins 12 |
| 3 to 12 months | Repeat PSA | A small early rise is expected as levels normalize 17 |
| Annual and ongoing | PSA plus prostate exam | A rise above about 1.4 ng/mL in a year, or a new nodule, triggers urology referral 1 |
Who should not take TRT
Some men should not start testosterone, or should be evaluated with extra caution first, and the prostate figures prominently on that list. Drawing on the Endocrine Society guideline and the FDA label, the situations that call for avoiding or deferring TRT include active, untreated, or suspected prostate cancer; a palpable prostate nodule or induration that has not been evaluated; a PSA above the guideline threshold pending workup (generally above 4 ng/mL, or above 3 ng/mL in men at higher risk); and male breast cancer 15. Consumer drug labeling lists the same prostate and breast cancer contraindications 12.
These are physician-evaluated findings, not a self-screening checklist. You are not meant to decide on your own whether a prostate finding disqualifies you; a proper evaluation before starting is what catches these situations. For men who turn out not to be candidates because of prostate concerns, there are other paths to discuss, including the non-testosterone options in our overview of TRT alternatives and endogenous-testosterone approaches such as enclomiphene, which raises the body's own testosterone through a different mechanism.
How TRT and prostate risk is evaluated and monitored
Pulling the threads together, prostate safety on TRT is a process, not a single decision. Before starting, a clinician confirms genuinely low testosterone on more than one morning blood test, then establishes a prostate baseline with a PSA measurement and a digital rectal exam where age-appropriate 12. That baseline both screens for a prostate problem that would change the plan and gives a reference point for every later PSA reading.
After starting, PSA and a prostate exam are repeated on a schedule, commonly within the first three to twelve months and then periodically once stable 1. A PSA that rises faster than expected, or a new nodule, sends a man to urology rather than triggering panic. For any man with a prostate cancer history, monitoring is tighter and the decision is shared with his specialists 211. It is why TRT is a supervised treatment, not a supplement you manage alone.
Frequently Asked Questions
For men with documented low testosterone, current evidence does not show that TRT causes new prostate cancer. The largest dedicated trial found no significant difference in prostate cancer rates between testosterone and placebo (0.46 percent versus 0.42 percent) 3, and major cancer centers agree that appropriately used testosterone therapy does not appear to raise the risk 67. The real caution is a cancer that already exists, not a new one being started.
TRT does not appear to increase overall cancer risk, and testosterone does not plant new tumors 8. The nuance is that the prostate is a testosterone-sensitive tissue, so an existing prostate cancer can be fueled by testosterone, which is why active disease is a contraindication. Male breast cancer is the other hormone-sensitive contraindication on the label 512.
It can be, in carefully selected men, but it is not a blanket yes. A 2025 scoping review supports cautious, supervised use after curative treatment while noting that long-term data are limited 11, and the AUA calls it a shared decision because the evidence is not strong enough to quantify the risk precisely 2. Candidates typically have low-risk, treated disease and a stable or undetectable PSA, with the decision made by a urologist or oncologist 9.
TRT may slightly increase prostate volume, but it does not appear to worsen urinary symptoms in most men. A review of 35 studies found that mild lower urinary tract symptoms improved or stayed unchanged on TRT 10. Men with severe urinary symptoms were less studied, so if you already have significant symptoms, mention them to your clinician before starting.
Usually yes, because testicular cancer is not androgen-driven, so testosterone does not fuel it the way it can fuel prostate cancer. Testicular cancer treatments such as orchiectomy and chemotherapy often cause low testosterone, and TRT is commonly used to treat that resulting deficiency rather than being avoided. As always, the decision is made with your oncology team based on your levels and recovery.
Usually only a little. Expect a small PSA rise in the first three to six months as testosterone normalizes, followed by stabilization 7. Clinicians watch for a change beyond that, such as a rise above about 1.4 ng/mL within a year or a new abnormal exam, which prompts a urology workup rather than an automatic diagnosis 1. This is why PSA is checked before and during therapy.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432.
- Bhasin S, et al. Prostate Safety Events During Testosterone Replacement Therapy in Men With Hypogonadism (TRAVERSE prostate sub-study). JAMA Netw Open. 2023;6(12):e2348692.
- Morgentaler A, Traish AM. Shifting the Paradigm of Testosterone and Prostate Cancer: The Saturation Model. Eur Urol. 2009;55(2):310-320.
- U.S. Food and Drug Administration. AndroGel (testosterone gel) prescribing information. 2025.
- Mayo Clinic. Testosterone and prostate cancer: What's the connection? Accessed 2026.
- Harvard Health Publishing. Appropriate use of testosterone therapy does not appear to raise prostate cancer risk. 2024.
- MD Anderson Cancer Center. Does testosterone cause cancer? Accessed 2026.
- Cleveland Clinic. Testosterone Replacement Therapy (TRT). Accessed 2026.
- Sexual Medicine Society of North America. TRT Doesn't Cause or Worsen Enlarged Prostate Symptoms (Kathrins et al., Urology, 2015 review). Accessed 2026.
- Testosterone replacement therapy following definitive treatment for prostate cancer: a scoping review. Int J Impot Res. 2025.
- MedlinePlus. Testosterone Topical. U.S. National Library of Medicine. Accessed 2026.
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.