
Does HRT help with hair loss? For many women the answer is a qualified yes: hormone replacement therapy can slow or stop menopausal hair thinning, and it produces partial regrowth for some, but it is not an FDA-approved hair loss treatment and the result depends heavily on which hormones are in your regimen. Estrogen tends to support hair, some progestogens can quietly work against it, and the same drop in estrogen that thins the scalp can coarsen hair on the chin and lip. So the honest version of "will HRT help with hair loss" is that HRT and hair loss are genuinely linked, but the outcome is not automatic. This guide walks through what each hormone does, whether HRT can cause hair loss, why some women shed more after starting it, and the realistic timeline for regrowth.
| Quick fact | What it means |
|---|---|
| Female pattern hair loss affects roughly 40% of women by age 50 | Midlife thinning is common, not a personal failing [7] |
| Estrogen extends the anagen (active growth) phase of the hair cycle | Losing it lets more hairs shift into shedding [2][3] |
| Minoxidil is the only treatment FDA-approved for female pattern hair loss | No form of HRT is approved specifically for hair [7] |
| Judge HRT's effect on hair at 3 to 6 months, not sooner | The hair cycle is slow, and early shedding can mislead you [1][3] |
🔑 Key Takeaways
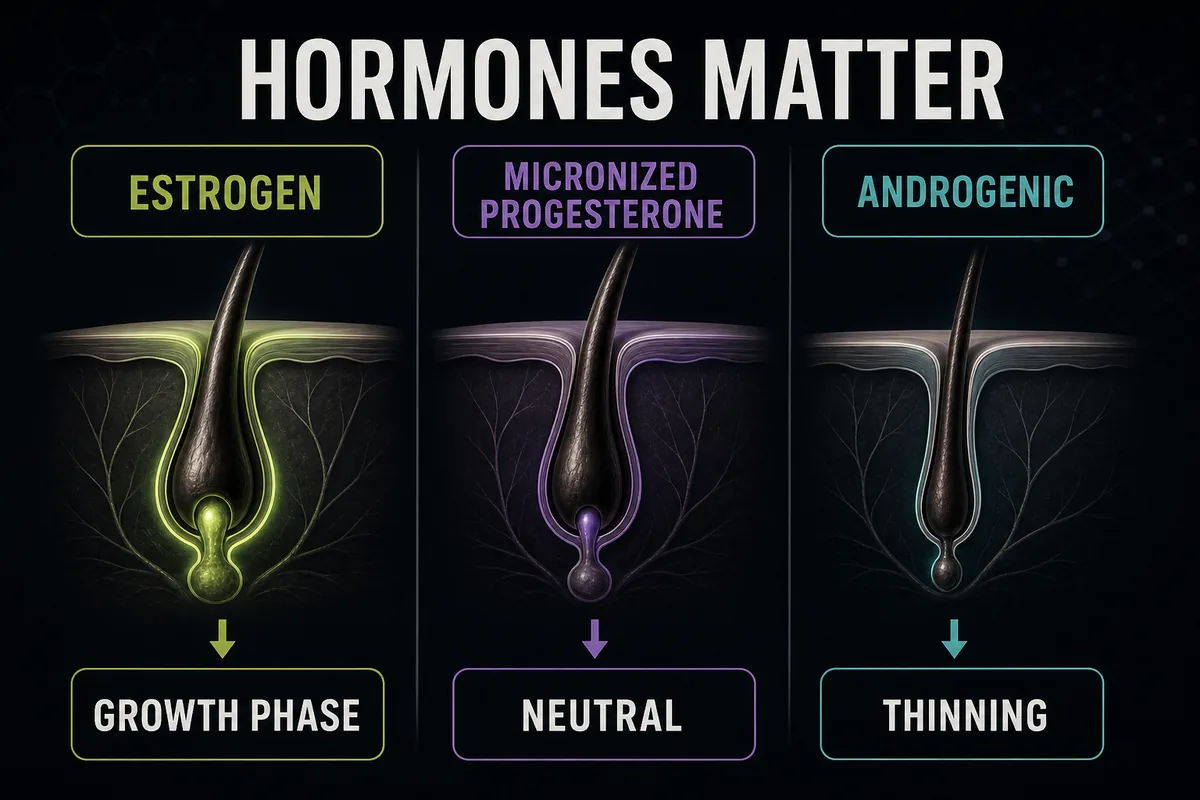
- Estrogen helps hair, so estrogen-based HRT often supports it. By extending the growth phase and raising SHBG, estradiol tends to protect and thicken thinning hair [1][3].
- Androgenic progestins can hurt. Synthetic progestogens such as norethindrone acetate and levonorgestrel can act on the follicle and worsen thinning; micronized progesterone is the hair-friendlier choice [1].
- Give it 3 to 6 months minimum. A temporary shed in the first weeks is common, and real density changes only show up months later [1][3].
- Transdermal estradiol plus micronized progesterone is the hair-friendliest combo, because it delivers steady estrogen without an androgenic progestin [1][5].
- Rule out thyroid and iron first. An underactive thyroid and low ferritin are common midlife causes of shedding that HRT will not fix [4][9].
Why Menopause Causes Hair Thinning
Every hair on your head runs through a cycle. It grows for years in the anagen phase, briefly transitions in the catagen phase, rests in the telogen phase, and finally sheds in the exogen phase before the follicle starts a new hair. Estrogen lengthens the anagen phase, which is why hair often looks its fullest during pregnancy, when estrogen is high, and why so many women notice thinning once estrogen falls at menopause [2][3].
As estrogen declines, the balance between estrogen and androgens tips toward the androgens. In genetically susceptible follicles, testosterone is converted by the enzyme 5-alpha reductase into dihydrotestosterone (DHT), and DHT gradually shrinks the follicle in a process called miniaturization. Each cycle produces a finer, shorter, less pigmented hair until the follicle stops producing a visible hair at all [4]. This is female pattern hair loss (FPHL), also called androgenetic alopecia.
The pattern in women looks different from men. Instead of a receding hairline and bald crown, women usually keep the frontal hairline but notice a widening part, reduced density over the crown, and a thinner ponytail [7][9]. It is a diffuse thinning rather than distinct bald patches.
It also matters whether your shedding is hormonal or not. Telogen effluvium is a temporary, heavy shed triggered by stress, illness, surgery, crash dieting, or a change in medication, and it usually recovers on its own once the trigger passes. HRT mainly helps the hormonal type of loss, the estrogen-and-androgen-driven FPHL, and does little for a telogen effluvium that is being driven by something else [4]. That distinction is why the first step is always working out what kind of hair loss you actually have.
HRT and Hair Growth: What Each Hormone Does
The question of HRT and hair growth is really three separate questions, because estrogen, progesterone, and testosterone each act on the follicle differently. Understanding does HRT help hair growth means looking at them one at a time.

Estrogen (estradiol)
Estrogen is the hormone doing most of the helpful work. It extends the anagen growth phase, supports follicle size, and keeps more hairs growing at once rather than resting or shedding [2][3]. Estradiol also raises sex hormone binding globulin (SHBG), a protein that binds circulating testosterone and lowers the amount of free testosterone available to be converted into DHT at the follicle [1]. The pregnancy analogy is the easiest way to picture it: the thick, glossy hair many women enjoy in pregnancy is an estrogen effect, and the shed that follows delivery is what happens when estrogen drops. Menopause is a slower version of that same withdrawal.
Progesterone
Progesterone's role depends entirely on which progestogen you take. Micronized progesterone, the body-identical form, appears to mildly inhibit 5-alpha reductase, meaning less testosterone is converted to DHT [1]. That is why the type of progestogen matters far more for hair than simply whether one is included. A regimen can contain progesterone and still be hair-friendly, as long as it is the right kind.
Testosterone
Testosterone is the double-edged one. It is sometimes added to HRT for low libido, and where a woman is genuinely deficient it has a role, but in DHT-sensitive women a testosterone add-on can thin scalp hair and coarsen facial hair [1][10]. It is worth knowing that most women with female pattern hair loss have normal circulating androgen levels; their follicles are simply more sensitive to normal amounts of androgen, so the issue is sensitivity rather than excess [4][10].
Can HRT Cause Hair Loss?
Yes, HRT can cause hair loss, though it is listed as an uncommon side effect rather than a typical one [6]. There are three main ways it happens.
First, and most importantly, the progestogen. Androgenic synthetic progestins such as norethindrone acetate and levonorgestrel can bind androgen receptors at the follicle and worsen thinning in susceptible women [1]. This is the single most common reason a regimen makes hair worse, and it is usually fixable by switching the progestogen.
Second, a temporary telogen shed. Starting HRT, or changing the dose, can push a batch of follicles into the resting phase, producing a shed roughly one to three months later. This is self-limiting and usually settles as your body adjusts [1][3].
Third, testosterone add-on therapy, for the DHT reasons described above [1].
So can HRT cause hair loss? It can, but the same tools that cause it, the choice of hormone and dose, are also what fix it. If you want the wider picture of what else HRT can do to your body, our full guide to HRT side effects covers the complete list. Hair is just one entry on it, and rarely the dominant one.
Taking HRT, Why Is My Hair Loss Worse?
If you are taking HRT and wondering why your hair loss is worse, you are not imagining it, and you are not stuck with it. Most cases come down to two things: a transitional shed in the first few months, or an androgenic progestin in the regimen. Work through the checklist below before you conclude that HRT has failed you.
Troubleshooting checklist: hair got worse after starting HRT 1. Check the progestogen. If it is norethindrone (norethisterone) acetate or levonorgestrel, ask your prescriber about switching to micronized progesterone. This single change resolves the problem for many women [1]. 2. Consider the timing. Shedding inside the first three months is often the transitional telogen shed, not treatment failure. It typically settles on its own [1][3]. 3. Look at dose fluctuation. Oral estrogen produces daily peaks and troughs; a transdermal patch or gel delivers steadier levels, which some women's follicles tolerate better [1]. 4. Get the basic labs. Ask about TSH (thyroid), ferritin (iron stores), and vitamin D before blaming the HRT. Thyroid disease and iron deficiency are common midlife causes of shedding that hormones will not fix [4][9]. 5. Watch for red flags. Scalp pain, burning, scaling, eyebrow loss, or rapid recession at the front can signal a scarring alopecia. Do not wait out the six-month HRT window; see a dermatologist promptly [7].
The key point is that "worse on HRT" is usually a solvable formulation or timing problem, not proof that hormones are wrong for you.
Best HRT for Hair Loss
Here is the honest starting point: no HRT is licensed or approved for hair loss, and no clinician prescribes hormones for hair alone [5][7]. Regimens are chosen to relieve menopausal symptoms and to fit your safety profile. That said, when hair is a real concern, there is a recognizable hair-friendliest pattern, and asking for the best HRT for hair loss is a reasonable conversation to have.
That pattern is transdermal estradiol (a patch, gel, or spray, for steady blood levels) combined, if you need a progestogen, with micronized progesterone, which has the lowest androgenic activity of the common options [1][5]. Body-identical hormones (estradiol and micronized progesterone) are structurally identical to what your body makes, whereas older synthetic progestins were designed for other properties and some carry androgenic activity that can work against hair [1].
Route matters, but mostly for safety rather than hair. Oral estradiol raises SHBG more than transdermal does, which in theory could help hair, but oral estrogen also carries a higher clot risk than transdermal, so the route is chosen on safety grounds, not hair grounds [5]. In practice the steadiness of a patch or gel is the more useful hair feature.
| HRT component | Common examples | Androgenic activity | Expected effect on scalp hair | Notes |
|---|---|---|---|---|
| Transdermal estradiol (patch, gel, spray) | Estradiol patch, estradiol gel | None | Supportive, steady blood levels | Route usually chosen on clot-risk grounds; the steadiest delivery |
| Oral estradiol | Estradiol tablets | None | Supportive, but with more day-to-day fluctuation | Raises SHBG more, but also raises clot risk versus transdermal [5] |
| Micronized progesterone | Prometrium (micronized progesterone) | Minimal, mildly anti-androgenic | Neutral to protective | Progestogen only needed with an intact uterus; the hair-friendly choice [1][5] |
| Norethindrone acetate | Found in some combined estrogen-progestin products | Higher | May worsen thinning in DHT-sensitive women | Switch candidate if hair worsens [1] |
| Levonorgestrel | Found in some combined patches and pills | Higher | May worsen thinning | Switch candidate if hair worsens [1] |
| Testosterone add-on | Off-label testosterone for women | Androgen | Can thin scalp hair, may coarsen facial hair | Prescribed for libido, not hair; off-label for women in the US [1][10] |
Qualitative ratings only; sources are Brough and Torgerson 2017 [1] and the Menopause Society 2022 position statement [5]. For the fuller landscape, see types of HRT explained, how HRT patches work, and bioidentical and body-identical HRT. If you want to see which clinics prescribe body-identical HRT online, you can compare the best online HRT clinics.
How Long Does HRT Take to Work for Hair?
Patience is the hardest part. A hair follicle works on a timescale of months, so nothing about does HRT stop hair loss can be judged quickly. Here is the realistic arc, and it is also the answer to whether HRT prevents hair loss over time: it protects follicles that are still viable, which is what "prevention" really means here.
HRT hair regrowth timeline
- Months 1 to 3: you may see a transitional shed as follicles resync. This is expected and does not mean the treatment is failing [1][3]. - Months 3 to 6: shedding usually stabilizes. The rate of loss slows before any visible thickening appears. - Months 6 to 12: if a density change is coming, this is when it becomes visible. Judge nothing before the six-month mark [1][3].
It helps to frame the goal correctly. HRT is far better at preservation than at restoration. It protects the follicles you still have and can thicken ones that are miniaturizing, but it does not resurrect follicles that have been dormant for many years [3]. That is also why timing matters: starting in perimenopause, while follicles are still active, tends to give a better hair result than starting a decade after menopause, when more follicles have already closed down. So can HRT reverse hair loss? Partially, and mostly for recently thinning hair, not for long-lost density.
One practical tip: track progress with a monthly photo of your part line in the same light, rather than examining the drain or the mirror every day. Daily checks reflect normal shedding noise; monthly photos reflect the trend. For how the medication ramps up across your whole symptom picture, see how long HRT takes to work overall.
HRT and Facial Hair: What Changes to Expect
The same androgen shift that thins scalp hair at menopause can coarsen hair on the chin and upper lip, which is why so many women ask about HRT and facial hair. As estrogen falls and the relative influence of androgens rises, some fine facial hairs turn darker and coarser [2][4].
So does HRT stop facial hair growth? Estrogen-containing HRT raises SHBG and reduces free androgen activity, and by rebalancing estrogen against androgens it can slow the development of new coarse facial hair [1][4]. That is the realistic version of will HRT stop facial hair growth: it can reduce the drive that creates new coarse hairs, and asking for the best HRT for facial hair concerns is, again, the estrogen-forward, non-androgenic pattern described above. What HRT does not do is remove hairs that are already established. Those need cosmetic approaches such as electrolysis, laser hair removal, or a prescription cream (eflornithine) to discuss with a clinician [9].
One caveat worth taking seriously: sudden or severe facial hair growth is not a simple menopause change and warrants an androgen workup rather than just an HRT tweak. Rapidly increasing coarse hair, especially with other signs of raised androgens, is a reason to see your clinician for testing [4][9].
What to Do if HRT Is Not Enough
HRT is one lever, not the only one, and for many women hair is best managed with a combination. If hormones alone are not doing the job, these are the evidence-based additions your clinician might discuss.
- Topical minoxidil (2% or 5%): the only treatment FDA-approved for female pattern hair loss. It needs at least six months of consistent daily use, and an uptick in shedding in the first few weeks is expected before regrowth, so do not stop early [7]. - Low-dose oral minoxidil: used off-label and managed by a dermatologist, it is an increasingly common option for people who cannot tolerate the topical form. - Spironolactone: an off-label anti-androgen sometimes used for FPHL in women, prescribed and monitored by a clinician. - Finasteride: relevant only for postmenopausal women, and not a first choice. A randomized trial found no benefit from 1 mg finasteride in postmenopausal women with androgenetic alopecia, so it is not the go-to option many people assume it is [8]. - PRP and low-level laser therapy: emerging options with growing but still limited evidence, offered by some dermatology clinics. - Nutrition and labs: check ferritin, vitamin D, and adequate protein intake, because deficiencies quietly worsen shedding. Note that biotin rarely helps if you are not deficient and can distort thyroid and other lab tests, so mention any biotin supplement before blood work [9].
Beyond hormones and drugs, some people also research adjacent options. For context on that, see the peptides studied for hair growth and our overview of peptide options studied for menopause. These are supporting reading, not a substitute for the FDA-approved and clinician-guided treatments above.
Frequently Asked Questions
Where to Go From Here
If your hair thinning sits alongside other menopausal symptoms such as hot flashes, disrupted sleep, or mood changes, HRT is worth a structured conversation with a clinician, because hair is rarely the only reason to consider it and rarely the strongest one. A good next step is to check whether your symptoms fit an HRT conversation, and if they do, to compare vetted online HRT clinics that prescribe body-identical options. For the full picture of benefits and risks, our cluster pillar, HRT for women: the complete guide, is the place to start.
References
- Brough KR, Torgerson RR. Hormonal therapy in female pattern hair loss. International Journal of Women's Dermatology, 2017;3(1):53-57. https://pmc.ncbi.nlm.nih.gov/articles/PMC5419033/
- Mirmirani P. Hormonal changes in menopause: do they contribute to a midlife hair crisis in women? British Journal of Dermatology, 2011;165 Suppl 3:7-11. https://pubmed.ncbi.nlm.nih.gov/21951457/
- Rinaldi F, Trink A, Giuliani G, Pinto D. The Menopausal Transition: Is the Hair Follicle Going through Menopause? Biomedicines, 2023;11(11):3041. https://pmc.ncbi.nlm.nih.gov/articles/PMC10604981/
- Ho CH, Sood T, Zito PM. Androgenetic Alopecia. StatPearls, NCBI Bookshelf. Updated 2024. https://www.ncbi.nlm.nih.gov/books/NBK430924/
- The Menopause Society (NAMS). The 2022 Hormone Therapy Position Statement. Menopause, 2022;29(7):767-794. https://menopause.org/professional-resources/position-statements
- NHS. Side effects of hormone replacement therapy (HRT). Accessed 2026. https://www.nhs.uk/medicines/hormone-replacement-therapy-hrt/side-effects-of-hormone-replacement-therapy-hrt/
- American Academy of Dermatology. Hair loss in women: female pattern hair loss. Accessed 2026. https://www.aad.org/public/diseases/hair-loss/types/female-pattern
- Price VH, Roberts JL, Hordinsky M, et al. Lack of efficacy of finasteride in postmenopausal women with androgenetic alopecia. Journal of the American Academy of Dermatology, 2000;43(5 Pt 1):768-776. https://pubmed.ncbi.nlm.nih.gov/11004621/
- Cleveland Clinic. Hair Loss in Women. Accessed 2026. https://my.clevelandclinic.org/health/diseases/16921-hair-loss-in-women
- Herskovitz I, Tosti A. Female pattern hair loss. International Journal of Endocrinology and Metabolism, 2013;11(4):e9860. https://pmc.ncbi.nlm.nih.gov/articles/PMC3968982/
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.