HRT or the pill for perimenopause is one of the most common crossroads women reach in their 40s, and the honest answer is that both can ease symptoms, but they are not interchangeable. The combined birth control pill uses a higher dose of synthetic hormones to switch ovulation off, so it also prevents pregnancy. Hormone replacement therapy (HRT) does the opposite job at a lower dose: it tops up the estrogen your ovaries are winding down on, but it is not contraception. Which one fits you depends on four things, your age, your main symptoms, whether you still need contraception, and your personal health history. This guide puts the two side by side so you and your clinician can weigh them for your situation.
🔑 Key Takeaways
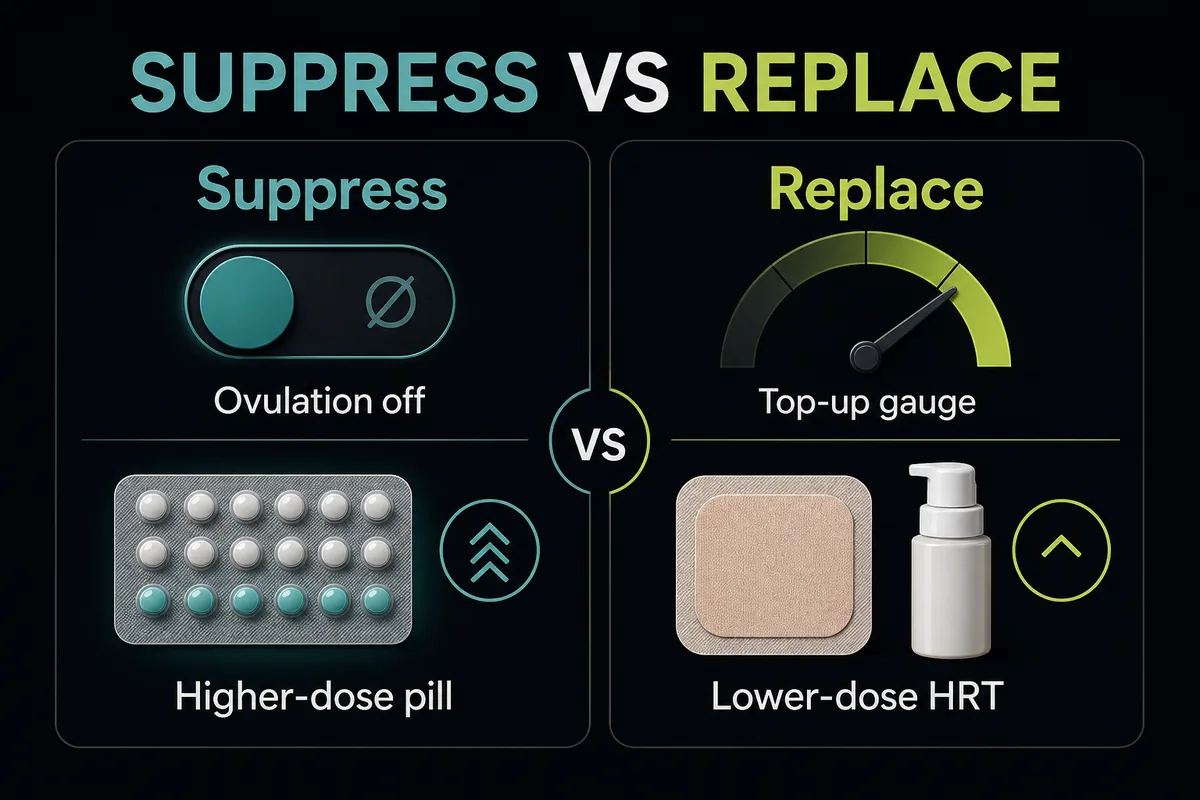
- The pill suppresses ovulation; HRT replenishes. A combined pill overrides your fluctuating ovaries with a steady, higher synthetic dose, while HRT simply replaces the estrogen you are losing at a lower dose [7][1].
- Only the pill prevents pregnancy. You can still ovulate and conceive on HRT until 12 months after your final period, so HRT is not birth control [6].
- Both protect bone and both carry a clot risk. Estrogen in either form supports bone density, and both raise clot risk, which climbs with smoking, high blood pressure, and age over 35 [1][3].
- Many women use the pill through their 40s, then switch to HRT. The pill handles heavy or erratic bleeding plus contraception; HRT usually takes over once contraception is no longer needed, often around menopause [7].
- Do not take the combined pill and HRT at the same time. Stacking two estrogen sources roughly doubles the exposure and the clot risk; progestogen-only methods can be paired with HRT instead [3].
What is the difference between HRT and birth control?
The difference between HRT and birth control starts with what each one is trying to do. A common question is whether birth control is HRT, or whether HRT is the same as birth control, and the short answer is no. Both contain an estrogen and (for most women) a progestogen, but they work at opposite ends of the hormone spectrum. Birth control suppresses your own hormone cycle and substitutes a controlled dose. HRT leaves your cycle alone and simply refills what is running low. That is why the difference between HRT and the contraceptive pill is often described as suppression versus replacement.
How the pill works in perimenopause
In perimenopause your ovaries do not fade smoothly. They sputter, so estrogen can swing high one week and low the next, which drives the erratic periods, hot flashes, and mood shifts of this stage [8]. The combined pill flattens those swings by suppressing ovulation and delivering a steady daily dose of synthetic hormones, usually ethinyl estradiol plus a progestin. Because it overrides your own ovarian output rather than supplementing it, the pill also does the second job HRT cannot: it prevents pregnancy.
How HRT works in perimenopause
HRT takes the opposite approach. It replenishes declining estrogen (paired with a progestogen if you still have a uterus, to protect the uterine lining) without switching ovulation off [1][2]. The dose is lower, the estrogen is typically estradiol that matches the hormone your body makes, and it comes in more forms than the pill: tablets, skin patches, gels, sprays, and vaginal preparations. If you want the deeper mechanics of using it at this stage, see our guide to HRT for perimenopause, and for a rundown of the delivery options, the types of HRT.
The single biggest mechanical difference is dose. The estrogen in a combined pill is far stronger than the estrogen in menopause HRT. By most estimates the pill delivers roughly 4 to 7 times the estrogen of a typical HRT regimen [7], and different sources put the range even wider, from about 2 times to 10 times depending on which products are compared. That dose gap is the reason the pill can shut ovulation down while HRT cannot, and it shapes almost every other difference below.
HRT vs birth control for perimenopause: side-by-side comparison
No competing page puts the full picture in one place, so here is the master comparison. This is birth control vs HRT across the factors that actually change the decision.
Birth control vs HRT for perimenopause: master comparison
| Factor | Birth control pill | HRT |
|---|---|---|
| Main purpose | Contraception plus symptom and cycle control | Replacing declining hormones to relieve symptoms |
| Hormone type | Synthetic ethinyl estradiol plus a progestin | Estradiol (often bioidentical) plus a progestogen if you have a uterus |
| Relative estrogen dose | Roughly 4 to 7 times higher [7] | Lower, replacement level |
| Suppresses ovulation | Yes | No [6] |
| Prevents pregnancy | Yes | No [6] |
| Cycle and bleeding control | Strong; can regulate or reduce heavy, erratic bleeding | Limited; not designed to control heavy bleeding |
| Best-fit stage | Earlier perimenopause, or when contraception is still needed | Later perimenopause and menopause |
| Available forms | Pill, patch, ring, plus IUD or implant for progestin-only options | Tablet, patch, gel, spray, vaginal |
| Typical stop or switch point | Around menopause, then switch to HRT | Individualized, reviewed with your clinician |
Sources: NCI, ACOG, The Menopause Society, PMC6165915, and PubMed 8605779 [7][6][1][2][3].
When you compare HRT vs birth control pills in perimenopause, three practical differences matter most. First, dose: the pill is the far stronger estrogen, which is why it carries the higher-dose risk profile of contraception. Second, contraception: only the pill prevents pregnancy, so if you still need birth control, that alone can settle the question. Third, cycle control: the pill can tame heavy or unpredictable bleeding, while HRT is built for symptom relief rather than bleeding control, and can itself cause some breakthrough bleeding, which we cover in bleeding on HRT.
Which is better for your perimenopause symptoms?
Neither wins across the board. The pill is stronger for bleeding and contraception, HRT is the gold standard for hot flashes and vaginal symptoms, and several concerns land closer to a tie. The table below breaks it down symptom by symptom.
| Symptom or need | Birth control pill | HRT |
|---|---|---|
| Irregular or heavy periods | Strong; regulates and often lightens bleeding | Limited; not a bleeding treatment |
| Hot flashes and night sweats | Helps by steadying hormone levels | Gold standard, the most effective option [1][2] |
| Mood changes | Can help by smoothing hormone swings | Can help, especially when linked to estrogen loss |
| Sleep | Better when driven by night sweats it controls | Better when night sweats are the cause [1] |
| Vaginal dryness | Limited effect | Effective, including low-dose vaginal estrogen [1][2] |
| Acne and skin | Often improves acne and skin | Neutral; not an acne treatment |
| Contraception | Yes, prevents pregnancy | No, not contraception [6] |
Sources: The Menopause Society and ACOG for symptom relief, plus PubMed 8605779 on contraception [1][2][6].
The pattern is clear. If your dominant problem is heavy, unpredictable bleeding or you still need reliable contraception, the pill covers more bases. If your dominant problem is hot flashes, night sweats, or vaginal dryness and you do not need contraception, HRT usually does more, at a lower hormone dose.
Benefits and risks by age
Age changes the math more than any single symptom does. The same combined estrogen that is routine at 42 can become a reason for caution at 52, and the risk questions shift as you move through the decade. None of the numbers below are meant to alarm you; they are here so you can weigh real, absolute risks rather than headlines.
In your early-to-mid 40s
For many women in their early to mid 40s who still need contraception and are dealing with heavy or irregular periods, the combined pill is often favored because it does both jobs at once. The important caveats are the standard contraindications to combined estrogen: smoking, high blood pressure, and migraine with aura all raise clot and stroke risk enough that clinicians usually steer away from combined estrogen contraception when they are present, especially after age 35 [3]. If any of those apply to you, a progestogen-only method or a non-hormonal option is often safer, and the conversation may move toward HRT sooner.
Late 40s to 50
As you approach 50, the higher pill dose gets a closer look. Many clinicians begin moving patients from the pill toward lower-dose HRT once contraception matters less, partly to reduce total hormone exposure. Delivery route also becomes part of the decision: transdermal estrogen (a patch, gel, or spray) is generally viewed as carrying less clot risk than estrogen taken as a tablet, which is one reason it is often preferred later in perimenopause and for women with clot risk factors [1].
Shared risks and protective effects
Both options share a similar core of risks and benefits. Both slightly raise breast cancer risk, and in both cases the absolute increase is small. For the pill, the modest rise appears to return toward baseline within about 10 years of stopping [9][4]. For combined HRT, the small increase is tied mainly to longer duration of use and is weighed against its symptom benefits [5]; you can read the fuller picture in our guide to HRT and breast cancer risk. The pill also has protective effects most people do not expect: it is linked to lower rates of ovarian, endometrial, and colorectal cancer [4]. And estrogen in either form supports the skeleton, which matters as bone loss accelerates around menopause, covered in protecting bone with HRT. Framed in absolute terms, the shared risks are small for most healthy women; the point is to match the option to your personal history rather than to an average.
Can you take the pill and HRT together?
Can you take the pill and HRT together? For the combined estrogen pill, the answer is generally no. Taking both means two estrogen sources at once, which roughly doubles your estrogen exposure and the clot risk that comes with it, so combining HRT and birth control of that type is not standard practice [3]. There is an important exception. Progestogen-only methods, such as the mini-pill or a hormonal IUD, can be used alongside estrogen HRT under a clinician's guidance, because they add contraception and (in the case of the IUD) can serve as the progestogen part of your HRT without stacking a second estrogen on top.
That raises a related question: does HRT work as birth control? It does not. Ovulation can still occur on HRT, so pregnancy remains possible until 12 months after your final period [6]. If you still need to prevent pregnancy while using HRT, you need a separate non-hormonal or progestogen-only method. In other words, HRT is not the same as birth control, and it does not replace it.
Switching from the contraceptive pill to HRT
Switching from the contraceptive pill to HRT is the part almost every other guide skips, yet it is where a lot of women get stuck. Here is how clinicians typically approach it, framed as general guidance rather than instructions to follow on your own.
When to consider switching. There is no single birthday that triggers the change. As a rule of thumb, many clinicians reassess somewhere around 50 to 55, but the timing is individualized [7]. The practical signals are that you no longer need contraception, or that the pill dose feels like more hormone than your symptoms require.
Why FSH testing is unreliable on the pill. A common instinct is to check a follicle-stimulating hormone (FSH) blood test to see whether you have reached menopause. The problem is that hormonal contraception suppresses that signal, and perimenopause is generally diagnosed from your age and symptoms rather than a single blood test, because hormone levels swing so much [10]. In practice, the pill can mask menopause onset, which is exactly why the switch is guided by symptoms and a clinician's judgment rather than one lab value.
How the switch is done in practice. Clinicians usually talk it through first, then choose a path: some use a pill-free interval or time an FSH check to get a clearer read, and some bridge the change with a hormonal IUD that provides both contraception and the progestogen arm of HRT while estrogen is added. The right sequence depends on your contraception needs and your health history.
What to expect. Because HRT is a lower dose than the pill, some women notice a temporary flare of symptoms during the transition, and it can take a little trial and adjustment to settle on the right dose and route. Some breakthrough bleeding during the change is common; persistent or unexpected bleeding is always worth reporting, as explained in bleeding on HRT.
How to decide: a simple framework
You do not need a quiz to narrow this down. Match your situation to the branches below, then take that starting point to your clinician, who will factor in your full history.
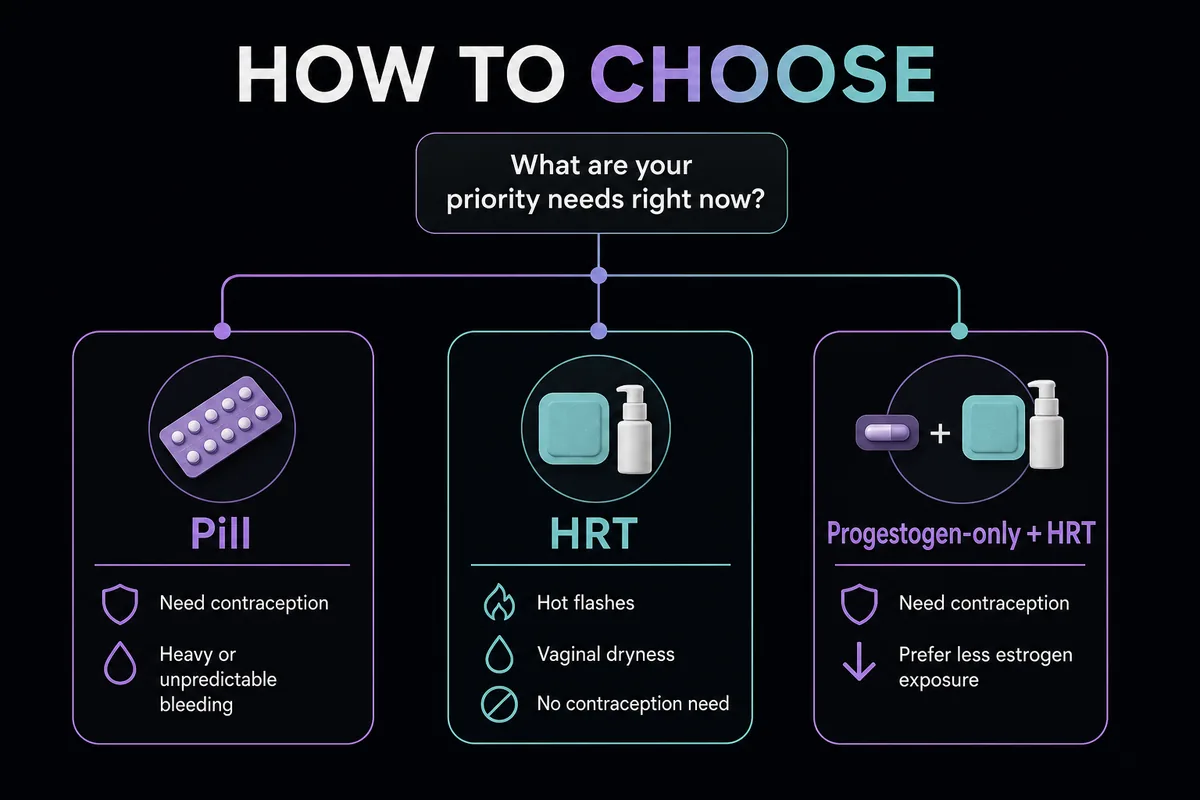
- The pill often fits if you still need contraception, your periods are heavy or unpredictable, you are under roughly 50, and you have low clot risk (no smoking, controlled blood pressure, no migraine with aura) [3]. - HRT often fits if your main problems are hot flashes, night sweats, or vaginal dryness, you no longer need contraception, or you have higher clot or blood pressure risk, in which case transdermal HRT is often the preferred route [1]. - A progestogen-only method plus HRT often fits if you need contraception but should avoid extra estrogen, for example a hormonal IUD paired with estrogen HRT [3].
Every branch ends the same way: discuss it with your clinician, because the right answer turns on your personal risk factors, not the averages. If you want to start that conversation from home, you can talk to an online HRT provider who can review your history and options. For broader background on the treatment itself, our overview of hormone replacement therapy for women is a good next read.
Frequently Asked Questions
References
- The Menopause Society. Hormone Therapy (patient education). The Menopause Society. https://menopause.org/patient-education/menopause-topics/hormone-therapy
- American College of Obstetricians and Gynecologists. Hormone Therapy for Menopause (FAQ). ACOG. https://www.acog.org/womens-health/faqs/hormone-therapy-for-menopause
- American College of Obstetricians and Gynecologists. Combined Hormonal Birth Control: Pill, Patch, and Ring (FAQ). ACOG. https://www.acog.org/womens-health/faqs/combined-hormonal-birth-control-pill-patch-ring
- National Cancer Institute. Oral Contraceptives and Cancer Risk. NCI. https://www.cancer.gov/about-cancer/causes-prevention/risk/hormones/oral-contraceptives-fact-sheet
- National Cancer Institute. Menopausal Hormone Therapy and Cancer. NCI. https://www.cancer.gov/about-cancer/causes-prevention/risk/hormones/mht-fact-sheet
- Gebbie AE, Glasier A, Sweeting V. Incidence of ovulation in perimenopausal women before and during hormone replacement therapy. Contraception, 1995. https://pubmed.ncbi.nlm.nih.gov/8605779/
- PubMed Central review (PMC6165915) noting combined oral contraceptive estrogen doses are higher than menopause hormone therapy regimens. Verify exact figure and citation details before publishing. https://pmc.ncbi.nlm.nih.gov/articles/PMC6165915/
- National Institute on Aging. What Is Menopause? NIA. https://www.nia.nih.gov/health/menopause/what-menopause
- American Cancer Society. Lifestyle-related Breast Cancer Risk Factors. American Cancer Society. https://www.cancer.org/cancer/types/breast-cancer/risk-and-prevention/lifestyle-related-breast-cancer-risk-factors.html
- Mayo Clinic Staff. Perimenopause: Symptoms and causes. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/perimenopause/symptoms-causes/syc-20354666
Disclosure: this article contains affiliate links to Gala Health. If you start care through them, we may earn a commission at no extra cost to you.