Can TRT cause ED? Sometimes, yes, but almost never because testosterone directly damages an erection. Erectile trouble or a flattened sex drive that shows up after starting testosterone is usually a fixable dosing or estrogen problem, a temporary dip after an early "honeymoon" phase, or a sign the erection problem was never hormonal in the first place. More often, testosterone replacement therapy does the opposite: in men with confirmed low testosterone it reliably raises desire and modestly improves erections. The catch, and the reason this question keeps men up at night, is that libido and erections are two separate systems, and TRT is far better at fixing one of them than the other. This page separates the two, puts real numbers on what testosterone can and cannot do, and walks through the handful of reasons erectile dysfunction while on TRT actually happens, all grounded in guideline and trial evidence rather than forum folklore.
Key Takeaways
- Desire and erections are different problems: desire (libido) is central and testosterone-driven, while an erection is a peripheral, blood-flow and nerve event, so TRT can lift one without fully fixing the other 58.
- TRT lifts libido reliably, erections only modestly: in confirmed low testosterone, trials show a clear jump in sex drive and sexual activity but a smaller erectile gain, roughly 2 points on a 30-point scale, versus much larger gains from PDE5 inhibitors like sildenafil 34.
- Four things explain ED that starts on TRT: estradiol too high, estradiol too low, a dose or timing that is off, or an erection problem that was never hormonal and TRT was never going to fix 17.
- Normal testosterone plus ED means TRT probably will not help: if your level is already in the normal range, raising it further usually does little for erections, and most erectile dysfunction is vascular 59.
- Morning wood is a rough dashboard light: losing or regaining it can signal how well your protocol, estrogen, sleep, and blood flow are lining up, not testosterone alone 68.
- Get labs, do not self-adjust: estrogen management, dose changes, and adding a PDE5 inhibitor are physician-directed decisions made from bloodwork, not something to tune from a message board 12.
Can TRT cause ED?
Directly, testosterone does not harm erectile tissue, so TRT is not "causing" erectile dysfunction the way a nerve injury or blocked artery would. When ED or low libido appears after starting, it is almost always one of four things: estradiol (a form of estrogen) running too high, estradiol pushed too low, a dose or injection rhythm that is not dialed in, or an erection problem with a non-hormonal root, usually vascular or psychological, that testosterone was never designed to treat 178. That is genuinely reassuring, because every one of those causes is identifiable with a lab panel and a conversation, and most are fixable.
It helps to name the pattern many men describe: sex drive and erections feel great for the first few weeks, then dip somewhere around weeks 6 to 12. That early lift is partly a real hormonal effect and partly the placebo and novelty of finally treating symptoms, and the later dip is often the body settling into a new equilibrium while estrogen and dose have not yet been optimized. It is a well-recognized "honeymoon then adjust" curve, not a sign that TRT broke something. Our guide to how long TRT takes to work covers that timeline in more detail.
Table 1. Four reasons TRT can be followed by ED or low libido
| Cause | What happens | Typical clue | Physician fix |
|---|---|---|---|
| Estradiol too high | Testosterone converts to estradiol, driving water retention, moodiness, and softer erections | Puffiness, nipple tenderness, unreliable erections | Check a sensitive estradiol assay, adjust dose or dosing frequency, occasionally a prescribed aromatase inhibitor 1 |
| Estradiol too low | Estrogen over-suppressed, which crashes libido and can affect orgasm | Flat desire, joint pain, trouble climaxing | Review dose or any aromatase inhibitor and let estradiol recover 1 |
| Dose or timing off | Peaks and troughs, or partial down-regulation of your own hormone signaling | Symptoms track the injection cycle | Labs, then a change in dose or how often it is given 12 |
| ED was never hormonal | A vascular or psychogenic erection problem is still present | Normal testosterone, risk factors like diabetes or high blood pressure | Screen for the real cause, treat it, often add a PDE5 inhibitor 58 |
Libido vs erections: two different problems
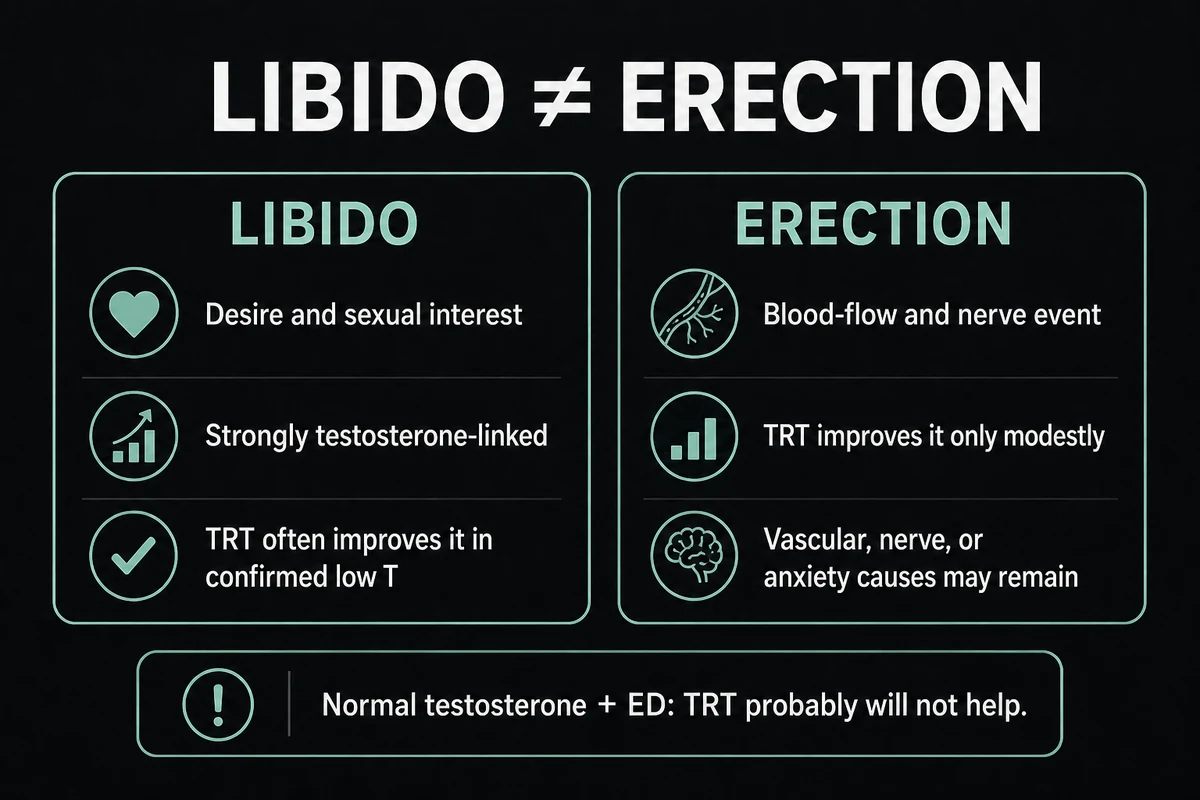
This distinction is the whole game, and getting it wrong is why so many men feel let down. Libido, meaning your sex drive and desire, is largely a central, brain-level phenomenon that testosterone strongly influences 68. An erection is a peripheral, plumbing-and-wiring event: the brain sends a signal, nerves release nitric oxide, arteries in the penis dilate, and blood fills and stays trapped. Testosterone supports that machinery, but it is not the machinery. If the arteries are furred up from diabetes or high blood pressure, or the nerves were damaged, or anxiety is slamming the brakes, all the testosterone in the world will not force a firm erection 59.
So testosterone can raise the wanting (desire) far more reliably than it restores the doing (a rigid erection). In the Testosterone Trials, a large placebo-controlled study in older men with low levels, testosterone gel clearly improved sexual desire and activity, with only a modest improvement in the erectile-function domain 3. A later systematic review and meta-analysis in confirmed hypogonadism found the same shape: a real but small erectile gain of roughly 2 points on the IIEF-EF scale (which runs 0 to 30), alongside a meaningful libido benefit 4. For comparison, PDE5 inhibitors such as sildenafil or tadalafil, the drugs built specifically for erections, typically produce much larger erectile gains, generally on the order of 6 to 8 points in their trials. That single contrast explains why men on TRT often still need an erection drug, and why WebMD notes that raising testosterone frequently is not enough for erections on its own 5.
Table 2. What TRT can and cannot fix
| Reliably improves (in confirmed low T) | Modestly improves | Does not fix on its own |
|---|---|---|
| Sex drive and desire | Erectile function (about 2 points on the 0 to 30 IIEF-EF scale) | Vascular ED (diabetes, high blood pressure, heart disease) |
| Energy and mood | Nerve-injury ED (after prostate surgery or spinal problems) | |
| Morning-erection frequency | Psychogenic or performance-anxiety ED | |
| Overall sexual activity | ED when testosterone is already in the normal range |
The takeaway is not that TRT is useless for erections. It is that TRT and libido are tightly linked, TRT and erections are loosely linked, and honest expectations prevent a lot of disappointment. Our page on TRT benefits covers the desire, energy, and mood gains in more depth.
Does TRT increase libido and sex drive?
Yes. In men with genuinely low testosterone and symptoms, raising the level back to a normal range is one of the most consistent things TRT does for sexual health: it increases desire, spontaneous interest, and overall sexual activity 346. The American Urological Association guideline reflects this, stating that testosterone therapy may improve erectile function and low sex drive in appropriately selected men (a Moderate recommendation, Grade B) 2. The Endocrine Society guideline likewise lists low libido and reduced sexual activity among the symptoms that should prompt a clinician to measure testosterone in the first place 1.
Timing matters for expectations. Desire tends to be one of the earlier things to shift, often within about 3 to 6 weeks, while any erectile improvement builds more slowly over several months 6. This is also where the honeymoon-then-dip pattern lives: an early surge in sex drive can partly settle as the initial novelty fades and the body finds its new baseline, which is normal and not a failure of treatment. Mayo Clinic frames the benefit carefully, noting that in men with documented low testosterone and sexual dysfunction, therapy can raise libido and erectile function, while the benefit is much less clear for the ordinary testosterone decline of aging 6. In other words, TRT to raise sex drive works best when the tank is genuinely low to begin with.
Why do some men get low libido on TRT?
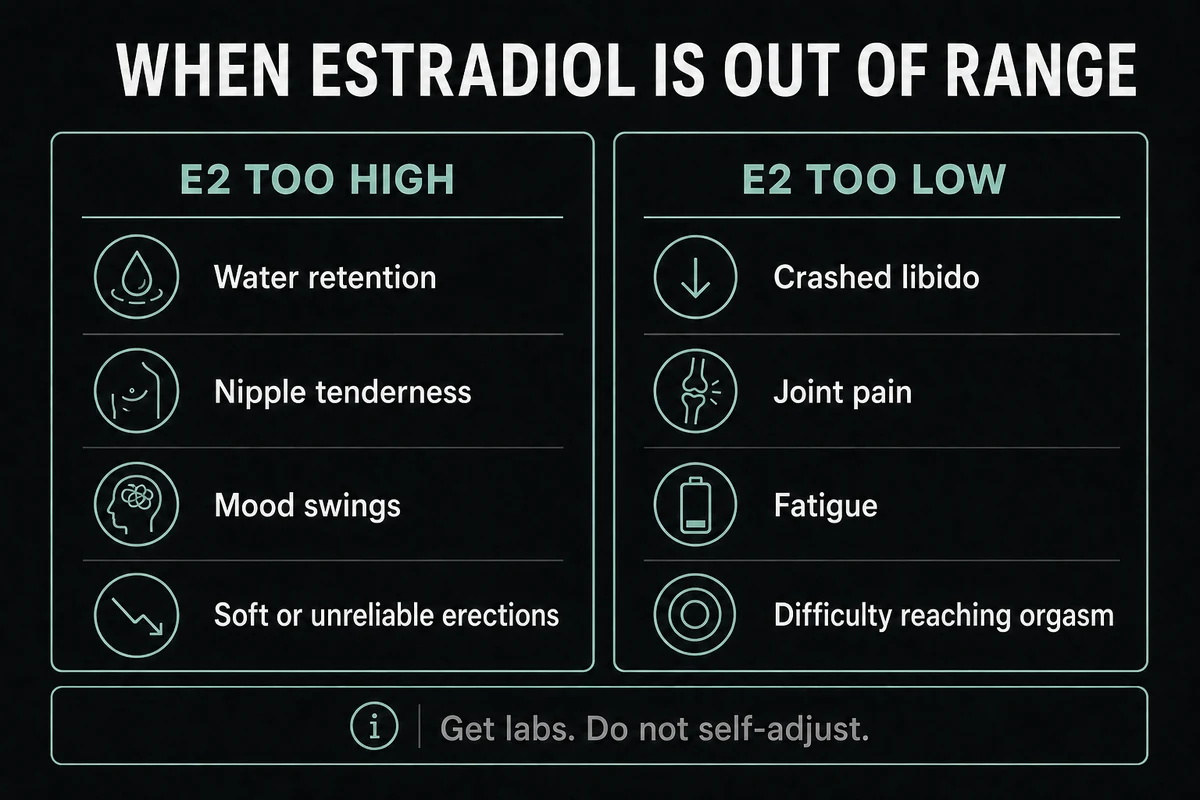
It feels like a cruel twist: you start testosterone to fix a flagging sex drive and end up with low libido on TRT instead. It happens, and the reasons are usually mechanical rather than mysterious. The most common culprit is estrogen. Because some testosterone naturally converts to estradiol, TRT can push estradiol too high, which paradoxically dampens erections and mood, or, if a clinician or a do-it-yourself protocol over-suppresses it, too low, which flattens desire and can cause joint pain and trouble reaching orgasm 1. Chasing "zero estrogen" is a classic mistake, because men need some estradiol for normal libido and sexual function.
Other drivers of low sex drive on TRT include a dose or schedule that leaves you crashing before the next injection, elevated prolactin (a different hormone worth checking), an underactive or overactive thyroid, poor sleep or untreated sleep apnea, chronic stress, and certain medications, especially SSRAI antidepressants, which are well known to blunt desire and orgasm. The honeymoon dip around weeks 6 to 12 also gets mistaken for a permanent loss of libido when it is really the settling-in phase. None of this is something to solve alone. Estrogen management in particular is physician-directed, because aromatase inhibitors are prescription drugs that cause the low-estradiol problems in the table below when misused. See our overview of TRT side effects for how estrogen shifts are tracked.
Table 3. High vs low estrogen (E2) signs on TRT
| High estradiol (E2) signs | Low estradiol (E2) signs |
|---|---|
| Water retention and puffiness | Crashed libido |
| Nipple sensitivity or tenderness | Joint pain and stiffness |
| Moodiness or emotional swings | Fatigue and low energy |
| Soft or unreliable erections | Difficulty reaching orgasm |
If your libido has dropped rather than risen, the fix usually lives in this differential, not in adding more testosterone. A dose review, a sensitive estradiol test, a prolactin and thyroid check, and an honest look at sleep and medications resolve most cases.
Erectile dysfunction while on TRT
Erectile dysfunction while on TRT deserves its own workup, because blaming testosterone is often the wrong move. When erections stay poor despite adequate testosterone, clinicians run a differential rather than simply raising the dose: is the dose or timing suboptimal, is estradiol too high or too low, is prolactin elevated, is the thyroid off, or, most importantly, is there an underlying vascular or metabolic problem 589? The last one is the big one. Most erectile dysfunction, on TRT or off it, comes down to blood flow, and conditions like diabetes, high blood pressure, high cholesterol, and cardiovascular disease damage the small arteries of the penis long before they announce themselves elsewhere 59. MedlinePlus is blunt that most erection problems have a physical cause, with low testosterone being just one of several 9.
That is why the honest sequence is to screen before you blame hormones. An erection problem that persists on well-optimized testosterone is a prompt to check cardiovascular and metabolic health, review medications (blood-pressure drugs, antidepressants, and antihistamines can all contribute), and consider psychological factors, not to keep pushing testosterone higher. The Endocrine Society guideline explicitly supports adding a PDE5 inhibitor when ED continues despite adequate testosterone, rather than treating testosterone as the sole lever 1. Getting your TRT dosage right is part of this picture, but it is rarely the whole answer for erections.
No morning wood on TRT
Waking up with no morning wood on TRT is one of the most common worries men raise, and it is a genuinely useful signal. Morning and overnight erections (clinicians call them nocturnal penile tumescence) depend on both adequate testosterone and healthy vascular and nerve function working together 8. When they disappear, it can point to estradiol being out of range, sleep debt or untreated sleep apnea (a big and underrated one, since these erections happen during REM sleep), a vascular issue, or an antidepressant. Because they are partly a non-conscious, blood-flow-driven event, their absence is a rough indicator of the plumbing, not just the hormone.
The flip side is encouraging: a returning morning erection is a decent, informal sign that a protocol is dialing in, that estradiol is landing in a reasonable window, and that the vascular side is cooperating. It is not a lab test, and it should not be over-interpreted, but many men and clinicians treat its return as a green light that things are moving in the right direction. If it stays absent, that is worth raising as part of the erectile workup above, not shrugging off.
Can TRT be used to treat ED?
TRT is a legitimate treatment for erectile dysfunction only when the ED is genuinely driven by low testosterone. When a man has confirmed, symptomatic low testosterone, correcting it can improve erections as part of the broader sexual benefit, which is exactly the scenario the guidelines endorse 12. The problem is that low testosterone is an uncommon cause of erectile dysfunction compared with vascular disease, so TRT is the right tool for a minority of ED cases, not the default fix.
Here is the honest de-selection: if your testosterone measures in the normal range and you have ED, raising it with TRT probably will not help, and both WebMD and Harvard Health say so plainly 57. Harvard notes that testosterone may increase desire but might not fix erections, and that hormonal low testosterone is an uncommon cause of impotence 7. Cleveland Clinic makes the same point from the other direction: low testosterone is one contributor to ED, but ED is usually multifactorial, with blood flow the first thing to investigate 8. So "TRT for ED" makes sense when a proper workup shows low testosterone; when testosterone is normal, the answer is to look at the vascular, neurological, medication, and psychological causes instead. A systematic review of testosterone treatment in men with low levels supports this sober framing: real benefits, but modest, not miraculous 12.
TRT plus PDE5 inhibitors and other options
Because testosterone and erection drugs work on different parts of the system, they are often used together under medical supervision rather than as either-or. PDE5 inhibitors (sildenafil, tadalafil, and similar) act directly on penile blood flow and produce the larger erectile gains, while TRT restores desire and supports the underlying tissue in men who are truly low 15. Combining a PDE5 inhibitor with testosterone is a recognized approach when low testosterone and erectile dysfunction coexist, and guidelines specifically endorse adding a PDE5 inhibitor when erections remain a problem despite adequate testosterone 1. There is also research interest in desire-specific options such as bremelanotide (PT-141), which works centrally on sexual motivation rather than on blood flow, for select cases. All of these are physician-directed prescriptions, chosen and dosed by a clinician, not a menu to assemble yourself.
For men whose libido and erectile complaints coincide with the testicular shutdown that TRT causes, there are fertility-sparing and HPG-preserving strategies worth discussing with a clinician. Options such as hCG, which keeps the testicular signaling active, or enclomiphene, which can raise the body's own testosterone without shutting the axis down, are sometimes relevant, and our guide to TRT and fertility explains how that suppression works and why it matters for some men's sexual symptoms. These are options to raise with your clinician, not a workaround to try on your own.
When to see your doctor and what labs to ask about
If your sex drive or erections change on TRT, the answer is testing, not tinkering. A sensible workup that your clinician may order includes total and free testosterone drawn in the morning (and confirmed with a second test, since a single reading can mislead), a sensitive estradiol assay, prolactin, and thyroid function, plus a look at the vascular and metabolic picture: blood pressure, blood sugar, and cholesterol 179. The Endocrine Society is clear that testosterone should be measured only in men with symptoms and consistently low levels, confirmed on more than one occasion, which is why the second morning test matters 17.
Two safety points close this out. First, do not self-adjust your dose or start an aromatase inhibitor on your own to "manage estrogen," because pushing estradiol too low creates the exact low-libido, joint-pain, and orgasm problems you were trying to avoid 1. Second, be aware that treatment rules and labeling shift over time; in early 2025 the FDA updated testosterone product labels class-wide, removing the older boxed cardiovascular warning and adding a blood-pressure warning, which is one more reason monitoring belongs with a clinician 11. Prescription testosterone also carries a transference caution with gels and other real label-level effects worth reviewing 10. The right move for any change in sexual function is a conversation and a lab panel, not a forum protocol.
Frequently Asked Questions
Not directly, but ED can follow starting TRT for one of four fixable reasons: estradiol too high, estradiol too low, a dose or timing that is off, or an erection problem that was never hormonal (usually vascular or psychological) and was never going to respond to testosterone 18. Each of these is identifiable with labs and a clinical review, and most are correctable.
Yes. In men with confirmed low testosterone, raising the level reliably increases sex drive and sexual activity, and it is one of the most consistent benefits of treatment 34. Desire often shifts within about 3 to 6 weeks, though an early surge can settle somewhat as the body reaches a new baseline 6.
The usual suspects are estrogen out of range (too high or over-suppressed too low), a dose that crashes before your next injection, elevated prolactin, thyroid problems, poor sleep, stress, or antidepressants, plus the normal honeymoon-then-dip pattern around weeks 6 to 12 1. It is a physician-guided workup, not a reason to simply add more testosterone.
Morning and overnight erections need both adequate testosterone and healthy blood flow and nerves, so losing them can signal estradiol imbalance, sleep debt or sleep apnea, a vascular issue, or an antidepressant rather than testosterone alone 68. A morning erection that returns is a rough sign the protocol is dialing in.
Only when the ED is driven by genuinely low testosterone; in that case correcting it can help as part of the broader sexual benefit 12. If your testosterone is already in the normal range, TRT probably will not fix your erections, because most ED is vascular, and a PDE5 inhibitor or treating the underlying cause is usually needed 57.
In men with low, symptomatic testosterone, yes, TRT to raise sex drive is well supported, and guidelines note improvements in low sex drive with therapy 24. The benefit is much less predictable when testosterone is already normal, where a low sex drive more often has other causes worth investigating 6.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432 (amended).
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (Testosterone Trials). N Engl J Med. 2016;374(7):611-624.
- Corona G, et al. Testosterone replacement therapy and sexual function in men with hypogonadism: a systematic review and meta-analysis. 2023 (PubMed 37589949).
- WebMD. Low Testosterone and Erectile Dysfunction. Accessed 2026.
- Mayo Clinic. Testosterone therapy: Potential benefits and risks as you age. Accessed 2026.
- Harvard Health Publishing. Is testosterone therapy safe? Take a breath before you take the plunge. April 2024.
- Cleveland Clinic. Does Low Testosterone Cause Erectile Dysfunction? Accessed 2026.
- MedlinePlus. Erection problems. U.S. National Library of Medicine. Accessed 2026.
- MedlinePlus. Testosterone Topical. U.S. National Library of Medicine. Accessed 2026.
- U.S. Food and Drug Administration. FDA issues class-wide labeling changes for testosterone products. February 2025.
- Huo S, et al. Treatment of Men for Low Testosterone: A Systematic Review. PLoS One. 2016;11(9):e0162480 (PMC5031462).
The information in this article is for educational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting any new supplement or compound. Results vary by individual.