


Cagrilintide peptide has a clear job.
It makes the amylin pathway matter again. That is why people search for cagrilintide by itself, then immediately ask about CagriSema, semaglutide, tirzepatide, weekly dosing, side effects, and 5mg vial math.
🔑 Key Takeaways
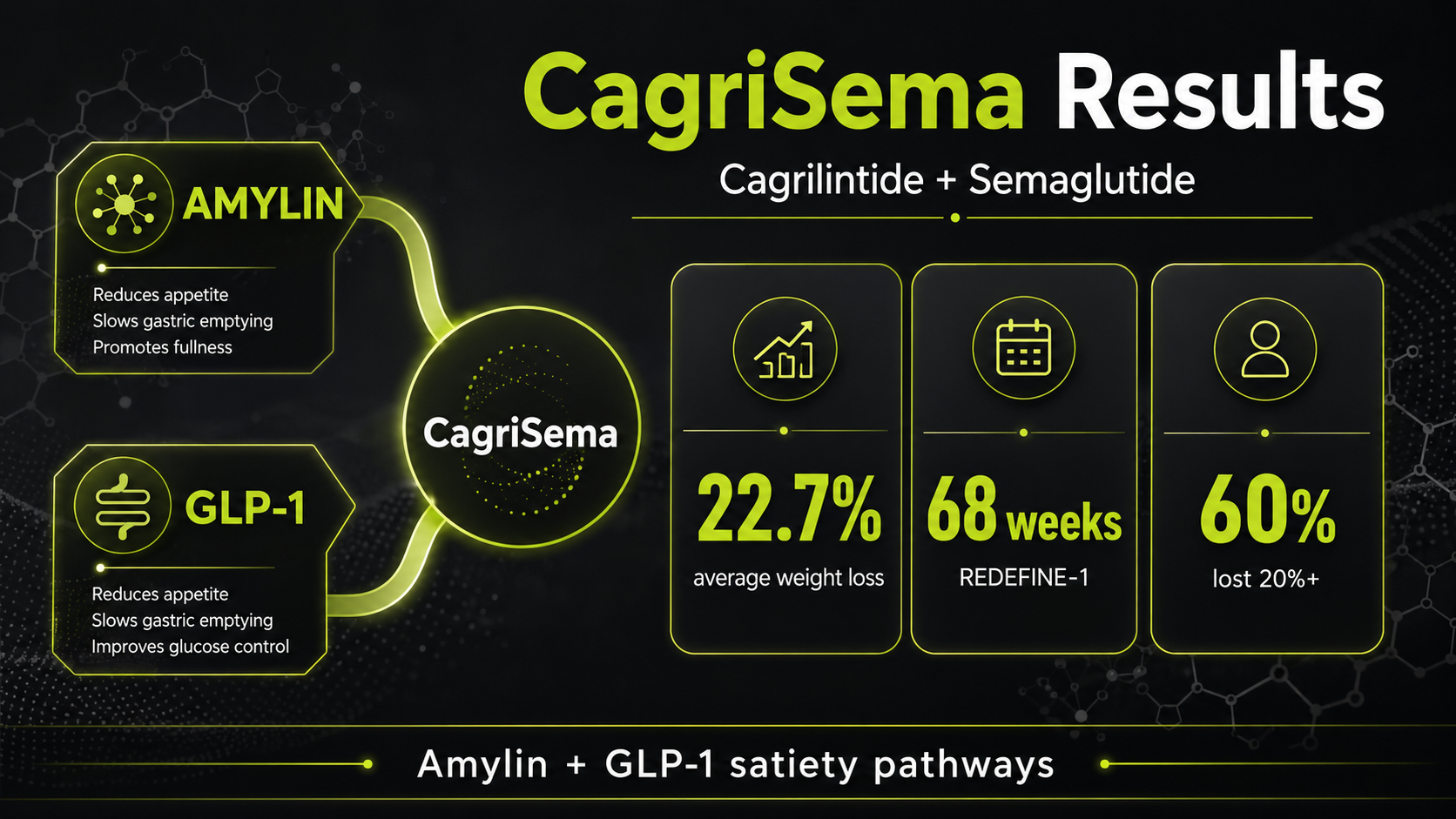
- Cagrilintide peptide is a long-acting amylin analogue. It works through a different satiety pathway than GLP-1 drugs like semaglutide.
- The biggest ranking intent is not just "what is it?" Readers want CagriSema results, weekly dose escalation, reconstitution math, and comparison against tirzepatide.
- In REDEFINE 1, CagriSema produced 22.7% average weight loss at 68 weeks when all participants stayed on treatment, versus 16.1% with semaglutide and 11.8% with cagrilintide alone.
- In REDEFINE 4, CagriSema reached 23.0% weight loss at 84 weeks, but tirzepatide 15mg reached 25.5%, so CagriSema did not beat tirzepatide in that head-to-head trial.
- The main limiting side effects are nausea, vomiting, constipation, and appetite suppression that becomes too strong. Slow titration matters more than chasing the highest dose quickly.
This page is built as the all-in-one cagrilintide peptide guide: what it is, how it works, what the trial results actually show, how dosing is usually escalated, how 5mg vial calculations work, and where it fits next to semaglutide, tirzepatide, and retatrutide.
What Is Cagrilintide Peptide?
It is an amylin analogue.
Cagrilintide, also known as AM833, is a long-acting version of amylin. Amylin is a hormone released with insulin after meals. Its job is to help the body register fullness, slow stomach emptying, reduce post-meal glucagon, and make a smaller meal feel like enough.
That makes cagrilintide different from the peptides most people already know. Semaglutide is a GLP-1 receptor agonist. Tirzepatide activates GIP and GLP-1. Retatrutide activates GIP, GLP-1, and glucagon. Cagrilintide is built around amylin receptor activity, which is why it is being developed both alone and as the amylin half of CagriSema.
CagriSema is the fixed-dose combination of cagrilintide 2.4mg and semaglutide 2.4mg. That combination is the reason cagrilintide has become a top search topic: amylin plus GLP-1 produced stronger weight-loss data than either component alone in pivotal trials.
Plain-English version
GLP-1 drugs make hunger quieter. Cagrilintide adds a different fullness signal, especially around meal size and gastric slowing. The combination is powerful because the pathways overlap less than people assume.
How Cagrilintide Works
The pathway starts after meals.
Natural amylin helps the brain and digestive system understand that food has arrived. Cagrilintide extends that signal into a once-weekly peptide. The effect is not one single switch. It is a cluster of signals that makes eating less feel less forced.
The practical result is simple: cagrilintide is not trying to be another semaglutide. It brings in a second satiety pathway. That is the reason most serious comparisons focus on CagriSema rather than cagrilintide alone.
CagriSema Results: What Changed
The combination became the headline.
The top-ranking pages all talk about cagrilintide, but the deeper intent is CagriSema. Readers want to know whether amylin plus GLP-1 is meaningfully better than a GLP-1 alone, and whether it can compete with tirzepatide.
The honest read is not "CagriSema destroys everything." It does not. The direct tirzepatide comparison was humbling. But the data still make cagrilintide important because it shows that amylin can add clinically meaningful weight loss on top of semaglutide.
Cagrilintide Dosage and Titration
The dose should climb slowly.
Most cagrilintide searches eventually become dosing searches. The common target discussed in trials is 2.4mg once weekly, but the target dose is not the starting dose. The starting dose is low because stomach-related side effects are usually the reason people stop early.
Some people need longer at each step. That is not failure. If nausea, vomiting, constipation, or low food intake becomes the main story, the next dose increase is usually the wrong priority.
Practical dose rule
The best cagrilintide dose is the dose someone can actually tolerate. A slower climb often beats a fast escalation that ends with skipped meals, dehydration, and stopping the peptide entirely.
If you are comparing this schedule with GLP-1 dosing, see the tirzepatide dosage chart and retatrutide dosing schedule. The shared theme is gradual escalation, but cagrilintide's amylin effect makes meal-size tolerance especially important.
5mg Vial Reconstitution and Units
The vial math causes mistakes.
Many cagrilintide peptide pages mention dosing but skip vial math. That gap matters because a 5mg vial can mean very different syringe units depending on how much bacteriostatic water is added.
The table below uses a U-100 insulin syringe, where 100 units equals 1mL. Always confirm the vial amount, water volume, syringe type, and intended dose before drawing anything. For a calculator-style walkthrough, use the peptide reconstitution guide.
That is why 2.0mL is commonly discussed for a 5mg vial: it keeps the lower doses easy to measure while keeping the 2.4mg dose just under one full U-100 syringe. Adding more water may make low doses easier to fine-tune, but it pushes the target dose beyond a single 100-unit draw.
How Cagrilintide Is Usually Injected
The route is usually subcutaneous.
In trials, cagrilintide and CagriSema are given once weekly under the skin. Common injection areas are the abdomen, thigh, or upper arm. Rotating sites matters because repeated use of the same small area can increase irritation and make absorption less predictable.
People also ask whether cagrilintide should be taken with food. The once-weekly schedule is not meal-timed like some short-acting medications. The bigger issue is food volume after the dose. Heavy, greasy meals are more likely to feel bad when gastric emptying is slowed.
- Use the same weekday when possible.
- Rotate injection sites each week.
- Avoid large meals during dose increases.
- Prioritize fluids and protein when appetite drops.
- Do not increase dose while side effects are still active.
Cagrilintide Side Effects
The stomach is the bottleneck.
Most cagrilintide side effects come from the same mechanism that makes it useful: delayed stomach emptying and stronger fullness. The effect can be helpful when meals are too large, but it can feel rough if the dose rises faster than the digestive system can adapt.
For a deeper side-effect breakdown, read our cagrilintide side effects page. The short version is this: side effects are usually dose-escalation problems before they are maintenance problems.

Cagrilintide vs Semaglutide
They are different satiety signals.
Semaglutide is the GLP-1 benchmark. Cagrilintide does not replace it in the current data. Instead, it adds an amylin signal that can strengthen the total effect when combined.
| Feature | Cagrilintide | Semaglutide | What It Means |
|---|---|---|---|
| Main receptor pathway | Amylin | GLP-1 | Different satiety biology |
| Typical trial schedule | Once weekly | Once weekly | Easy to combine in a fixed-dose product |
| Standalone weight-loss signal | About 11.8% at 68 weeks in REDEFINE 1 | About 16.1% at 68 weeks in REDEFINE 1 | Semaglutide is stronger alone in that trial |
| Combination outcome | 22.7% with CagriSema at 68 weeks | Amylin adds to GLP-1 rather than duplicating it | |
| Main tolerability issue | Fullness, nausea, constipation | Nausea, constipation, diarrhea | GI management matters for both |
If you are comparing GLP-1 options more broadly, start with our GLP-1 peptides for weight loss overview.
Cagrilintide vs Tirzepatide
The direct head-to-head changed expectations.
Before REDEFINE 4, many readers expected CagriSema to clearly beat tirzepatide because the REDEFINE 1 results looked so strong. The direct comparison was more complicated. CagriSema reached 23.0% weight loss at 84 weeks, but tirzepatide 15mg reached 25.5% in the same open-label trial.
That does not make cagrilintide irrelevant. It means the positioning is more specific. Cagrilintide is not automatically the strongest next-generation option. Its value is the amylin pathway, the CagriSema combination, and the possibility of higher-dose combinations now being studied.
Best read on the data
CagriSema looks clearly stronger than semaglutide alone, but it did not beat tirzepatide 15mg in REDEFINE 4. That is the nuance most thin articles miss.
Cagrilintide vs Retatrutide
This is a pathway comparison.
Retatrutide targets GLP-1, GIP, and glucagon receptors. Cagrilintide targets the amylin system. That makes them very different tools, even though both are discussed in the same weight-loss peptide searches.
For the retatrutide side of that comparison, see what is retatrutide and our retatrutide vs tirzepatide comparison.
Who Cagrilintide Fits Best

It fits a specific problem.
Cagrilintide makes the most sense when meal size, constant appetite, or GLP-1 plateau is the main frustration. It is less compelling as a standalone option if someone simply wants the strongest available single-agent weight-loss data.
- GLP-1 plateau: The amylin pathway may add a different satiety signal when GLP-1 response has flattened.
- Large meal size: Stronger fullness and gastric slowing may help people who still eat large portions on GLP-1 therapy.
- Food noise: Some users report fewer snack urges, though individual response varies.
- Diabetes plus weight focus: REIMAGINE data make the combination interesting for type 2 diabetes discussions.
- Low tolerance for nausea: This is the caution group. Cagrilintide may be a poor fit if GI side effects already limit GLP-1 use.
The decision should not be based on hype alone. It should be based on the specific appetite problem, tolerance history, medication access, and clinician guidance.
Storage, Timing, and Missed Doses
Consistent weekly timing reduces confusion.
Lyophilized peptide vials are typically kept cold and protected from light before mixing. After reconstitution, many peptide users store the vial refrigerated and use it within a limited window. Exact storage depends on the product source, sterility, preservative, and instructions supplied with the vial.
The weekly dose day should be easy to remember. If a dose is missed, do not double the next dose without medical guidance. With long-acting weekly peptides, stacking doses too close together can make side effects worse several days later.
Common Cagrilintide Mistakes
Most cagrilintide mistakes are predictable.
- Escalating while nauseous: If the current dose is not tolerable, the next dose is unlikely to fix it.
- Eating normal large meals: Delayed emptying makes large meals feel worse than expected.
- Ignoring constipation early: Once constipation becomes severe, it is harder to correct.
- Mixing vial math in your head: Write down vial size, water volume, concentration, and units.
- Comparing only headline percentages: REDEFINE 1 and REDEFINE 4 answer different questions.
Frequently Asked Questions
Sources
- Novo Nordisk REDEFINE 1 headline results, December 2024
- Novo Nordisk CagriSema US regulatory submission, December 2025
- Novo Nordisk REDEFINE 4 headline results, February 2026
- Novo Nordisk REIMAGINE 2 headline results, February 2026
- Novo Nordisk Annual Report 2025, CagriSema and cagrilintide update
- Once-weekly cagrilintide dose-finding trial, The Lancet, 2021